
How Adult Outpatient Treatment Supports Your Career

Key Takeaways
- Adult outpatient treatment lets working professionals protect their careers while recovering, with employment treated as a clinical outcome rather than a lifestyle bonus.2
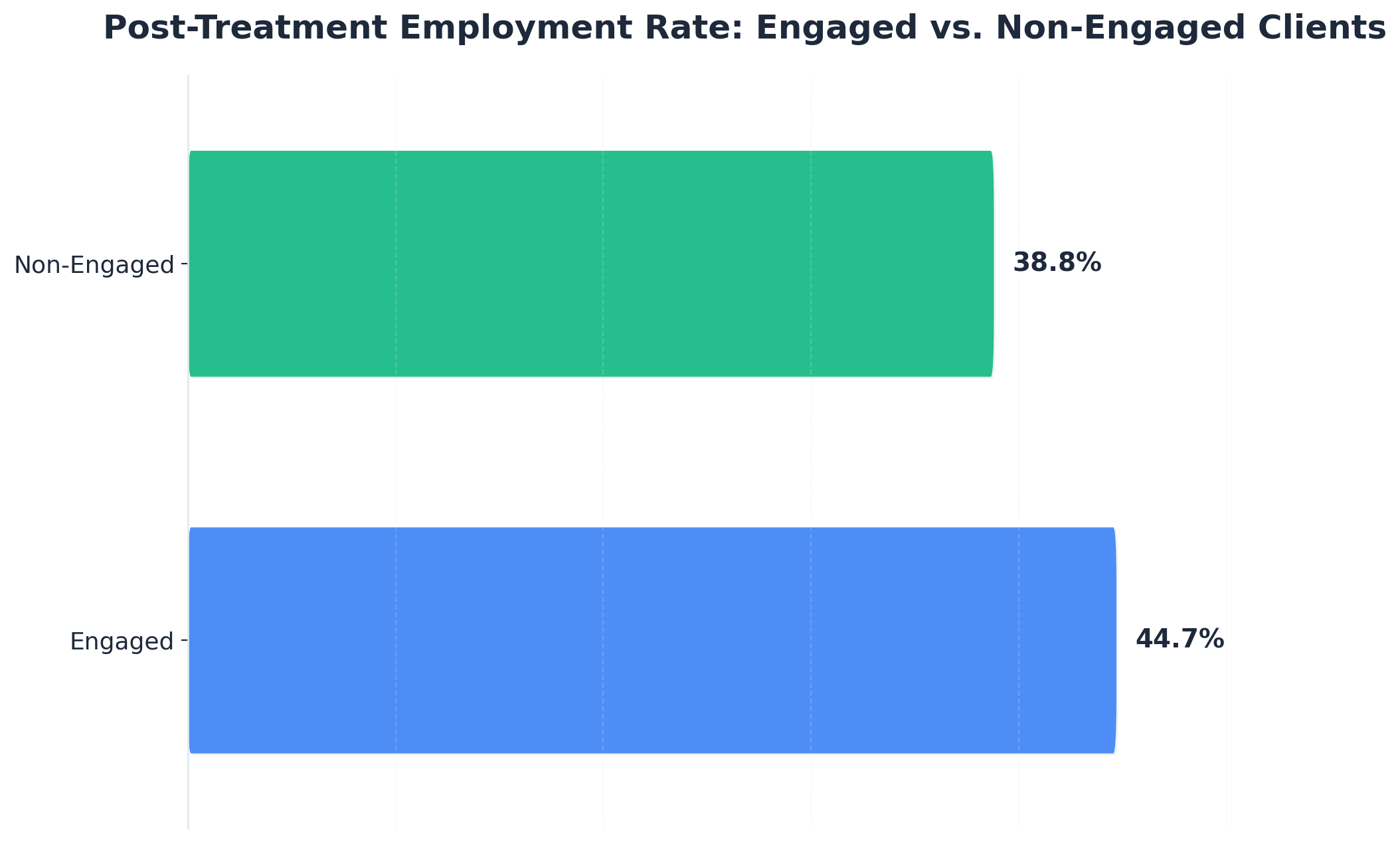
- Engagement, not setting, drives results — engaged outpatient clients showed 44.7% post-treatment employment versus 38.8% for non-engaged peers.1
- Staying in treatment for at least 90 days correlates with better employment, higher earnings, and housing stability, so durability matters more than intensity.3
- When choosing a program, press on travel protocols, clinician stability, telehealth integration, and how the team handles week eight — not just intake week.
The quiet calculation behind your search
You probably opened this tab after everyone else went to bed. Maybe you closed your laptop, picked up your phone, and typed the words you have been avoiding for weeks. That counts. That is already a kind of courage, even if it does not feel like one yet.
The question underneath your search is not really does outpatient treatment work. You are doing a quieter math problem. Can you get help without losing the career you spent twenty years building? Can you sit in a session on Tuesday evening and still be sharp in a Wednesday morning meeting? Can you protect your license, your clients, your team, your kids' tuition, and your own privacy, all at the same time?
Here is the honest answer: yes, more often than the cultural picture of "rehab" suggests. Adult outpatient treatment is not the consolation prize for people who are not sick enough for residential care. For working professionals, it is frequently the more durable choice, because your job is not the obstacle to recovery. Your job, your routine, your sense of who you are at work, can actually be part of what holds the recovery in place. Employment is treated as a clinical outcome in the research literature, not a lifestyle bonus.2
This article is written for the version of you reading at 11:47 p.m. with a calendar full of obligations tomorrow. We will walk through what a real week looks like, what shows up where, what to say and to whom, and what the evidence actually supports. No labels. No lectures. Just the information you came here to find.
Why staying at work is a clinical advantage, not a compromise
There is a story you may have absorbed, mostly from movies and a few cautionary tales at conferences, that real recovery requires disappearing for a while. Pack a bag, draft a vague email about a "family matter," and reappear thirty days later as a new person. For some people, in some situations, that is the right call. For most working professionals, it is not.
The clinical literature treats employment as a recovery outcome in its own right, not a side effect of getting better. That framing matters. It means the work you are afraid of losing is part of what your care plan is trying to protect, not something to be set aside until you are "ready." Your calendar, your competence, your reason to be up and dressed by 7 a.m., your sense of being useful to someone other than yourself — these are recovery assets.2
Here is the data point that quietly changes the conversation. In an NIH analysis of clients in outpatient substance use treatment, those who actively engaged in their program were employed at a rate of 44.7% after treatment, compared to 38.8% for clients who did not engage. The study also found that engagement increased the likelihood of employment by an additional 6 percentage points among clients with prior criminal justice involvement. A few caveats worth holding: this was a specific NIH sample, the overall main effect for engagement was modest, and the strongest lift showed up in the justice-involved subgroup. So this is not a promise that outpatient treatment will guarantee your job. It is evidence that showing up and doing the work inside an outpatient program is the variable that moves employment outcomes — not whether you went somewhere residential first.1
Read that twice. The format is not the lever. Engagement is the lever.
That should be a relief. It means you do not have to choose between credible care and your career. The CDC's workplace guidance points in the same direction: a recovery-supportive approach lowers the barriers to seeking and continuing care, including staying at or returning to work during treatment. The old framing — that you must hit some imagined bottom and vanish to get well — is not what the evidence describes. Your continuity at work is not the thing you are sacrificing for recovery. In a lot of cases, it is the thing helping you build it.5
The 90-day rule that quietly shapes everything else
If there is one number worth tattooing on the inside of your planner, it is ninety. Ninety days of staying in treatment is the threshold researchers keep landing on as the point where outcomes start to compound. The University of Washington's Addictions, Drug & Alcohol Institute puts it plainly in their retention toolkit: remaining in substance use treatment for at least 90 days correlates with an increased likelihood of employment, increased earnings, and housing stability.5
Three things, all at once. Your job. Your paycheck. The roof over your head. That is not a marketing slogan. It is what the retention research keeps showing.
Notice what that finding does not say. It does not say you have to be inpatient for ninety days. It does not say you have to do nine hours a week of group therapy for ninety days. It says you have to stay. The cadence — whatever cadence you and your clinician build around your work — has to last long enough for the new patterns to actually hold.
This is where outpatient care has a quiet structural advantage for someone in your position. A residential stay measured in weeks ends, and then you are on your own to build a maintenance routine inside a life you have not lived in a month. Outpatient treatment lets you build that routine inside the life you are already living. The ninety-day clock starts running while you are still answering emails, still running your Tuesday team meeting, still picking up your kid from practice.
That is also why the early weeks feel deceptive. Two or three sessions in, you may feel sharper, sleep better, and quietly wonder if you have already done the hard part. You have not. The hard part is week eight, when the calendar is full and a client crisis lands the same afternoon as your group, and the easiest thing in the world is to push the session by "just this once." Once becomes twice. Twice becomes a month of skipped work, and the ninety-day clock effectively resets.
So when you are evaluating programs, ask less about intensity and more about durability. How does this team help you stay engaged through a quarter close, a deposition week, a board offsite, a flu, a fight with your spouse? What happens on the week you want to quit? A program built for working professionals expects those weeks. It plans for them. That planning, more than any single therapeutic modality, is what carries you across the ninety-day line.
What a real week looks like when you keep your job
Most of the fear about treatment lives in a vague mental image: a place you go, a thing you do, a hole in your calendar you cannot explain. Once you see what an actual week looks like on paper, the fear gets smaller. Not gone. Smaller.
There is no single right schedule. The format that fits a partner at a litigation firm with court dates is not the format that fits a surgeon with a Tuesday OR block or a founder pitching investors across three time zones. What follows is the menu, in plain terms, so you can stop guessing what you might be signing up for.
Standard outpatient, IOP, and concierge-coordinated care
Three structures cover most of what working professionals actually use.
Standard outpatient usually runs one to two sessions a week, often a mix of individual therapy and a single group. Total time commitment lands somewhere around two to four hours weekly. It is the lightest touch and the easiest to hide inside a normal calendar.
Intensive outpatient (IOP) typically asks for nine to fifteen hours a week, spread across three to five days. Sessions are usually two to three hours at a stretch, often clustered in mornings or evenings so people can keep working. It is more demanding but also where a lot of the early structural work happens.
Concierge-coordinated outpatient blends both. You may do one or two clinical sessions a week, plus telehealth check-ins, plus a care coordinator who handles the logistics around your schedule. The clinical hours can resemble standard outpatient, but the wraparound is heavier and built around your travel, your time zones, and your privacy.
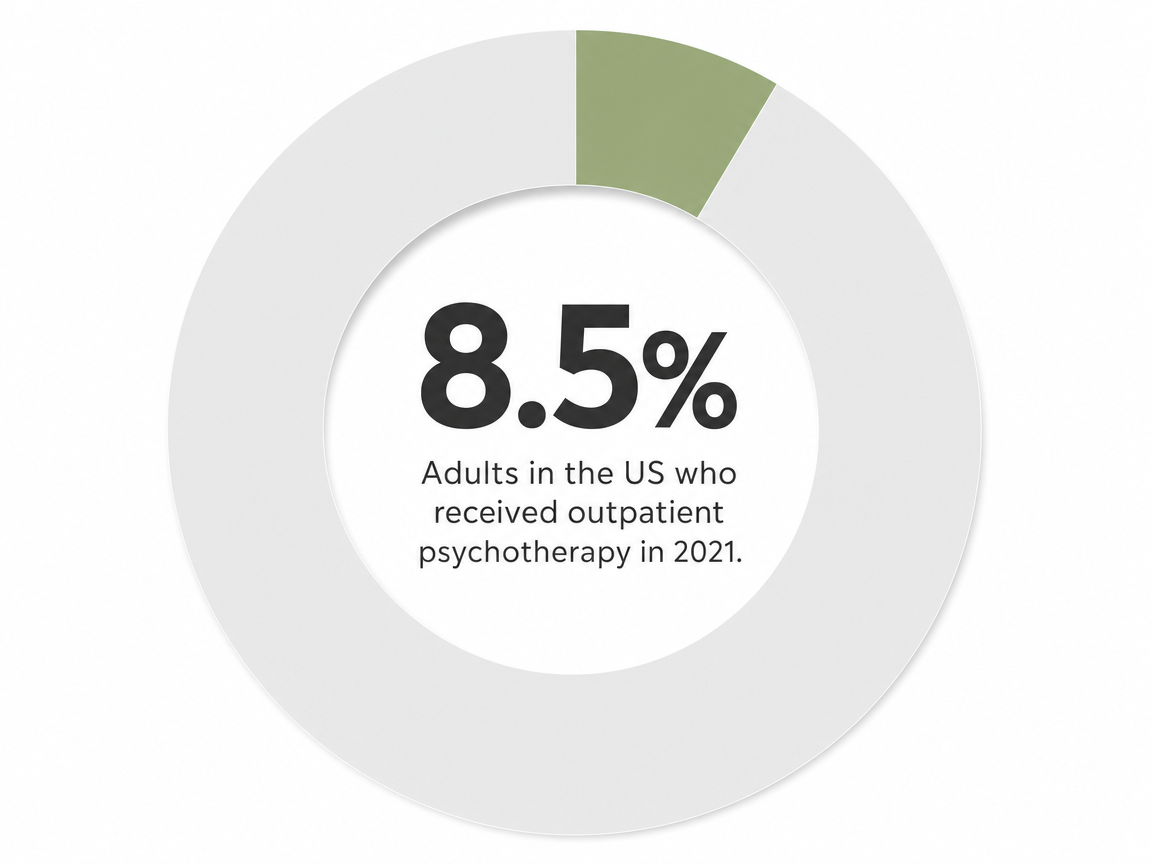
None of this is fringe. By 2021, 8.5% of U.S. adults had used outpatient psychotherapy in the past year — a meaningful jump driven partly by telehealth and partly by the fact that more people, including professionals, are quietly choosing it. You are not stepping outside the mainstream by picking outpatient care. You are stepping into it.6
Mornings, evenings, telehealth, and the calendar nobody has to see
Look at your week. Where are the soft edges?
For a lot of working professionals, the answer is a 7 a.m. block before the day starts, a 6 p.m. block after the last call, or a Friday afternoon that already runs slow. Good outpatient programs build around those edges instead of fighting your calendar. Individual therapy often lives in a fifty-minute window you can take from a closed office door or a parked car. Group sessions tend to land in early morning or evening tracks specifically so people can keep working.
Telehealth changed what is possible here. A session from your hotel room on a Wednesday night counts. A check-in from your home office between meetings counts. Your assistant sees a recurring "personal" block. Your team sees a manager who logs back in at 7:30 looking a little more rested than usual.
The calendar nobody has to see is not a trick. It is a schedule built by adults, for an adult life, that protects both the work and the recovery — exactly the kind of arrangement public health guidance now describes as recovery-supportive.5
Disclosure decisions: what to say, to whom, and when
Almost every professional reading this gets stuck on the same question, sometimes for months: who has to know?
The short answer is fewer people than you fear. Outpatient treatment was designed, in part, so the people in your professional orbit do not have to be informed about your medical care. You are an adult managing a health condition. The same privacy expectations that apply to a thyroid issue, a heart procedure, or a course of physical therapy apply here. The CDC's workplace guidance is explicit on this point: a recovery-supportive approach lowers barriers to seeking care, and that includes protecting the person's choice about disclosure.5
That said, there are a few decisions worth making on purpose, before someone else makes them for you. Who needs to know enough to cover for you on a Tuesday at 6 p.m. Who never needs to know at all. What language you use if a question comes up. The two pieces below sort the most common situations professionals walk into.
Your manager, your board, your clients
Default position: nobody at work needs a diagnosis. They need a schedule.
For a manager, "I have a standing medical appointment Tuesday and Thursday evenings, and a weekly Friday morning block for the next few months" is usually enough. You are not lying. You are giving them what they actually need, which is predictability. Most managers will not push past that, and the ones who do are not entitled to more.
Boards and clients are different animals. With a board, the question is fiduciary, not personal — are you fit to serve? In almost every case involving outpatient care, the answer is yes, and no disclosure is required. With clients, your contractual obligations control. If you can deliver the work on time, your medical calendar is your own.
One quiet truth: people often imagine the worst-case reaction and never test it. The conversation in your head is almost always harsher than the one across the desk.
Insurance, EAPs, and what actually shows up on a claim
Insurance is where the most disclosure anxiety lives, and where the reality is usually less dramatic than the fear.
A standard outpatient claim shows a date of service, a provider, and a billing code. It does not show your group therapy notes, your conversations with your therapist, or what you said on a Tuesday night. Your employer, in most arrangements, never sees individual claims at all. Federal privacy rules give substance use treatment records additional protection beyond standard health information.
Employee Assistance Programs (EAPs) are a separate question. EAPs can be a useful entry point for short-term counseling and referrals, and they are typically confidential by design. But the level of separation from your employer varies by program. If you want maximum distance from your workplace, paying out of pocket or using your health plan directly — without routing through the EAP — is the cleaner path. Ask the question before you start.
Travel, performance reviews, and the rest of professional life
Recovery does not pause for a quarterly board meeting. Neither does the rest of your professional life. The question is not whether the hard weeks will come. They will. The question is what you have built to absorb them.
Travel is the most common worry, and the most solvable. A standing Tuesday session becomes a telehealth session from a hotel room in Denver. A weekly group becomes a different group's evening track in your home city when your own provider is closed. Good outpatient programs build a travel protocol with you in week two, not week ten. Ask for it explicitly: what is the plan when I am on the road three nights a week in March?
Performance reviews are the second worry. Here is the part that surprises people. Most professionals doing real recovery work see their reviews hold steady or improve, not slip. Sleep returns. Mornings get cleaner. The low-grade panic that ate twenty percent of your attention quietly leaves the room. SAMHSA's employment-focused recovery guidance treats sustained work performance as a normal product of sustained care, not a happy accident. You are not getting better despite your job. The two are running on the same track.9
Then there are the rest of the unglamorous variables. The flu in February. A parent in the hospital. A merger. A divorce. Each one is a moment when skipping a session feels reasonable, and each one is exactly when the session matters most. Your care team should treat those weeks as the plan, not as exceptions. That is the difference between a program built around a working life and one built around an empty calendar.
Insight Beyond Treatment
At Next Level Wellness & Behavioral Health, we believe meaningful change starts with perspective, not just protocols.
That philosophy is directly led by Amanda Marino, whose voice in behavioral health extends beyond clinical settings into leadership, culture, and personal growth.
Through keynote speaking and live events, Amanda explores the deeper themes that show up in recovery, family systems, and life transitions: authenticity, resilience, accountability, and the courage to change. Her work invites audiences to move past labels and into honest conversations that create lasting impact.
Honest limits: outcomes are real, but not automatic
You deserve a straight answer here, not a brochure.
Outpatient treatment works for a lot of people. It also does not work the same way for everyone, and pretending otherwise would do you a disservice. In one study of formerly polysubstance users, 44.5% were employed at the time of follow-up. That is meaningful progress for a group that had been through a lot. It is also less than half. The number cuts both ways, and you should sit with both edges of it.8
What the research keeps pointing to is that good outcomes are real, but they are not handed out at intake. They are built. They are built by showing up the week you do not feel like it. By telling your therapist the truth about Saturday night instead of the version that sounds better. By calling your care coordinator before the missed session, not after. SAMHSA's employment-focused recovery framework is clear that sustained work outcomes come from sustained engagement with care, not from the act of enrolling.9
So here is the honest frame. If you do the work — the unflashy, repetitive, sometimes boring work of attending sessions, telling the truth, and staying connected through the hard weeks — adult outpatient treatment gives you a real chance at keeping the career and the life you have built, and improving both. If you stay half in, the data is less kind.
That is not a warning. It is permission to take this seriously and a reason to believe the effort is worth something.
Choosing a program that respects your professional life
By the time you start comparing programs, you have already done the hardest part. The next decision is narrower than it looks. Most outpatient programs use similar therapeutic models. The difference, for someone in your position, is whether the program is built around the assumption that you have a working life, or whether your working life is treated as an inconvenience to clinical scheduling.
A few things are worth pressing on before you sign anything.3,4
- Ask how the program handles the week you want to quit. Not the intake week. Week eight. Week twelve. What is the protocol when you miss a session, when you travel unexpectedly, when a crisis at work collides with a group you committed to? A program that cannot answer that in concrete terms is going to lose you somewhere around the ninety-day mark, which is exactly the threshold the retention research says you need to cross.
- Ask who actually answers the phone. A care coordinator who knows your travel schedule, your spouse's name, and the fact that you have a board meeting the third Thursday of every month is worth more than a brand-name modality on a website. Continuity of relationship is what makes the wraparound real.
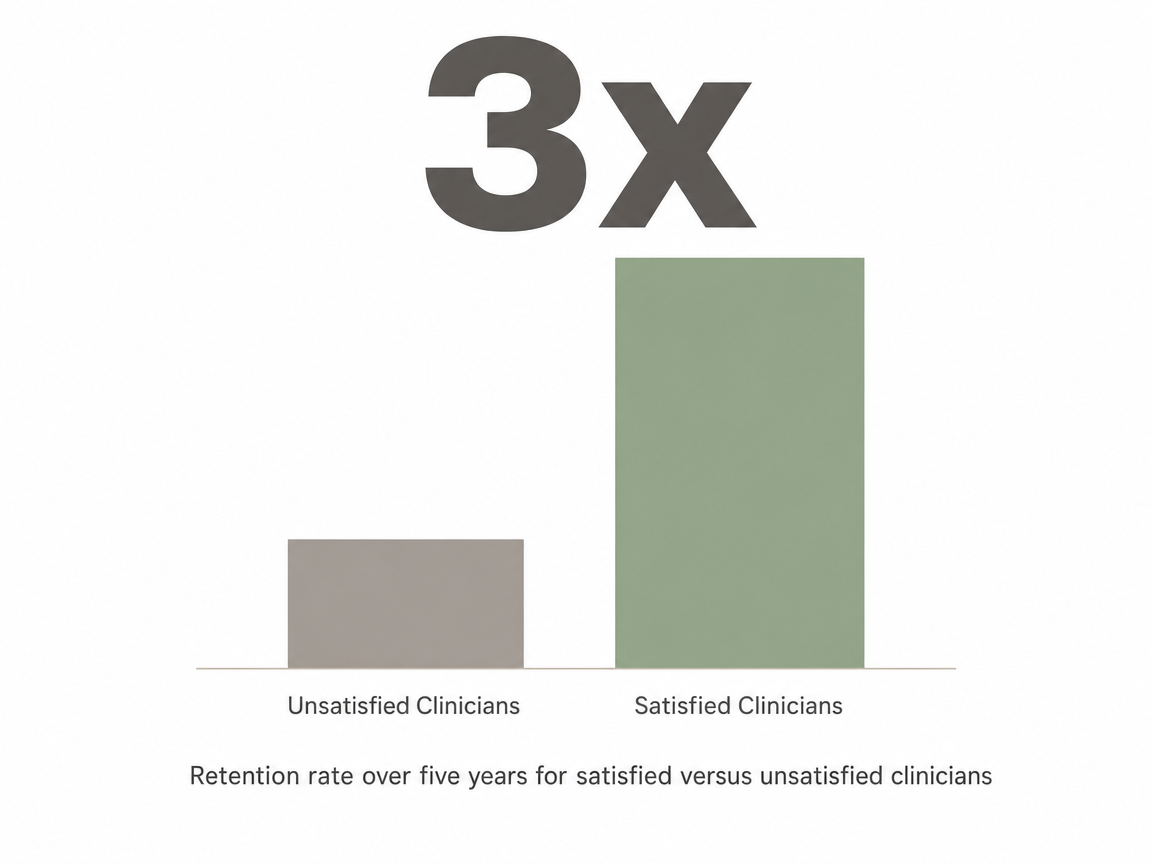
- Ask about clinician stability. The behavioral health workforce is under real pressure, and turnover affects your care. A 2025 analysis found anticipated five-year retention rates were nearly three times higher among clinicians satisfied with their work conditions. You do not need to interview the whole staff. You do need to ask, plainly, how long your primary therapist has been with the program and what happens if they leave mid-treatment.
- Ask how telehealth, in-person, and travel sessions weave together. A program that treats telehealth as a backup is a program that will quietly punish you for traveling. A program that treats it as a normal mode is one that has already adapted to professional life.
- And finally, ask what the first thirty days actually look like. Not the brochure version. The Tuesday-at-6-p.m. version. If the answer is specific, calm, and shaped around you instead of a fixed track, you are probably in the right room.
A first step that protects what you have built
You do not have to decide everything tonight. You only have to decide the next small thing.
That might be writing down the names of two people who could cover a Tuesday evening for you. It might be opening your calendar and looking, honestly, at where the soft edges are. It might be a single phone call tomorrow at lunch from a closed office door. None of these moves require you to label yourself, announce anything, or change who you are at work on Wednesday morning.
What the evidence keeps showing is that the people who do well in outpatient care are not the ones who came in with the most certainty. They are the ones who stayed long enough for the work to take, with a team that built the schedule around their actual life. That is a buildable thing. It starts with a conversation, not a commitment.3
If you want that conversation to be discreet, coordinated, and shaped around the career you have spent years building, that is the kind of support Next Level Wellness & Behavioral Health was designed to offer. When you are ready, the next step is a quiet one.
For support that meets you right where you are—anytime, anywhere—connect with us today.
Frequently Asked Questions
Can I really keep working full-time during outpatient treatment?
Yes, and that is the design intent. Standard outpatient runs roughly two to four hours a week, and intensive outpatient (IOP) typically lands between nine and fifteen hours a week, often clustered in early mornings or evenings so you can stay at your job. Public health guidance from the CDC explicitly supports staying at or returning to work during care. The key variable is consistent engagement with sessions, not whether you stepped away from your role.5
Will outpatient treatment show up on my insurance or background checks?
A standard insurance claim shows a date of service, a provider, and a billing code — not your therapy notes or what you discussed in group. Your employer typically does not see individual claims, and substance use treatment records carry additional federal privacy protections beyond standard health information. Outpatient psychotherapy itself has become common, with 8.5% of U.S. adults using it in 2021. Routine background checks do not access medical or treatment records.6
Do I have to tell my employer, board, or clients I'm in treatment?
In most cases, no. You are managing a health condition, and the same privacy norms that apply to other medical care apply here. A manager usually needs a schedule, not a diagnosis — "I have a standing medical appointment Tuesday evenings" is enough. Boards care about fitness to serve, which outpatient care rarely affects. Clients care about deliverables. The CDC frames this kind of discretion as part of a recovery-supportive approach that lowers barriers to care.5
How is outpatient treatment different from intensive outpatient (IOP) and residential care?
Standard outpatient is the lightest touch, usually one to two sessions weekly. IOP is more structured at nine to fifteen hours a week across three to five days, often built around work hours. Residential means living on-site for weeks at a time. The format matters less than engagement — an NIH study found post-treatment employment was 44.7% among engaged outpatient clients versus 38.8% among non-engaged clients. Showing up is what moves outcomes, not the setting.1
How long will I be in outpatient treatment?
Plan for at least ninety days as a starting frame. The University of Washington's retention research is consistent on this: staying in treatment for 90+ days correlates with better employment, higher earnings, and housing stability. Many professionals continue with reduced cadence — perhaps weekly individual therapy and a monthly check-in — for six to twelve months after that. Length depends on your situation, but the ninety-day threshold is where outcomes start to compound.3
What happens if I have to travel for work during treatment?
Travel is one of the most solvable parts of outpatient care. A standing weekly session becomes a telehealth session from your hotel room. Group can shift to a different evening track or a virtual format your provider supports. Ask any program directly, in week one, what their travel protocol is — what happens when you are on the road three nights in March, or across time zones for a deal. A program built for working professionals plans for that, not around it.
References
- ENGAGEMENT IN OUTPATIENT SUBSTANCE ABUSE TREATMENT AND EMPLOYMENT OUTCOMES. https://pmc.ncbi.nlm.nih.gov/articles/PMC3796147/
- Employment after beginning treatment for substance use disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC5830150/
- Overview of the Retention Toolkit - UW ADAI. https://adai.uw.edu/retentiontoolkit/overview.htm
- Job assessments and the anticipated retention of behavioral health clinicians. https://pmc.ncbi.nlm.nih.gov/articles/PMC12020279/
- Workplace Supported Recovery | Substance Use and Work - CDC. https://www.cdc.gov/niosh/substance-use/workplace-supported-recovery/index.html
- Trends in Adult Outpatient Psychotherapy in the United States, 2019-2021. https://pmc.ncbi.nlm.nih.gov/articles/PMC12771505/
- Transforming Lives Through Supported Employment (SE) Program. https://www.samhsa.gov/communities/criminal-juvenile-justice/grants-grantees/supported-employment
- Rate and Predictors of Employment among Formerly Polysubstance Users. https://pmc.ncbi.nlm.nih.gov/articles/PMC3416052/
- Substance Use Disorders Recovery with a Focus on Employment. https://www.samhsa.gov/resource/ebp/substance-use-disorders-recovery-focus-employment
- Substance Abuse, Behavioral Disorder, and Mental Health Counselors. https://www.bls.gov/ooh/community-and-social-service/substance-abuse-behavioral-disorder-and-mental-health-counselors.htm
- Engagement in outpatient substance abuse treatment and employment outcomes. https://pubmed.ncbi.nlm.nih.gov/23686216/
- Factors Influencing Turnover and Attrition in the Public Behavioral Health Workforce. https://pmc.ncbi.nlm.nih.gov/articles/PMC10756926/
- Substance Use Disorders - Statutes, Regulations, and Guidelines. https://www.samhsa.gov/substance-use/treatment/statutes-regulations-guidelines
A Voice Shaping the Conversation
The topics explored here—change, self-awareness, recovery, and growth—are the same themes Amanda Marino brings to audiences nationwide through speaking engagements and live events.
Known for her appearances on A&E’s Intervention and Digital Addiction, Amanda speaks to organizations, communities, and leadership teams about navigating adversity, embracing vulnerability, and building lives rooted in purpose. Her message resonates far beyond treatment, offering insight that applies to families, professionals, and anyone standing at a crossroads.



Heal on your terms—any time, anywhere.