
What Goes Into Effective Aftercare Planning?

Key Takeaways
- Post-discharge recovery functions as a chronic-care stage, not a finish line, so the plan should assume adaptation rather than deliver a one-time checklist 11.
- A real aftercare plan has five parts working together: a personal recovery map, scheduled checkups, case management, a written crisis protocol, and a daily behavioral routine.
- Scheduled outreach outperforms passive discharge, with structured checkups more than doubling days in specialty treatment and increasing abstinent days over three months 2.
- Draft the recovery map, name first-line crisis contacts, calendar the next four weeks of checkups, and identify who owns the logistics before adding anything else.
The Chronic-Care Phase Nobody Prepared You For
You finished treatment. Somebody handed you a folder, maybe a printed schedule, a few phone numbers, and a warm goodbye. And now you're here, standing in your own kitchen, trying to figure out what the next Tuesday actually looks like.
Here's what most people aren't told: the weeks after discharge aren't the ending of treatment. They're the start of a different clinical stage entirely. Researchers who study recovery describe it as a chronic-care process, closer to how you'd manage a long-term health condition than how you'd finish a course of antibiotics 11. That reframe matters, because it changes what you should expect from yourself and from the plan sitting in that folder.
SAMHSA describes recovery as a process of change where you improve your health, live a self-directed life, and work toward your own version of a full one 8. Not a finish line. A direction.
The transition window is real and specific. You lose the structure of scheduled days. You return to environments that still carry old associations. Your identity shifts, sometimes faster than the people around you can track. None of that means something is wrong. It means you're in a stage that deserves its own operating plan, not a discharge checklist stapled to good intentions. The rest of this guide walks through what that plan actually contains, and how it should change as you do.
Why a Discharge Checklist Isn't a Plan
A checklist is a snapshot. A plan is a system that keeps working when your Wednesday falls apart.
Most discharge paperwork gets built for the day you leave, not the ninety days after. It lists a therapist referral, a support group meeting time, maybe a psychiatrist follow-up, and a prescription refill schedule. Useful information. Not a plan. A plan tells you what happens when the therapist has a two-week wait, when the meeting time collides with a work trip to Denver, when a family event puts you in the same room as a former drinking friend, and when a Tuesday feels heavier than it should for no reason you can name.
Here's the honest version of what the research says. A meta-analysis of continuing care found a small but real positive effect at the end of treatment (g = 0.187) that actually grew larger at follow-up (g = 0.271) 10. Read that carefully. The benefit didn't fade. It compounded. That is the signature of a chronic-care process, not an epilogue. Small, steady, and cumulative.
That reframe changes what you should demand from your own plan. You don't need a document that guarantees an outcome. You need one that assumes you'll adapt, that expects the terrain to shift, and that has a next move built in for the moments a checklist doesn't cover. The following five components are what that looks like in practice, and they're what the rest of this guide walks you through.
The Five Components of a Real Aftercare Plan
A Recovery Map That Reflects Your Actual Life
Start with the map, not the meetings. A recovery map is a written document that describes what your life is trying to look like over the next twelve months and what has to be true for that life to hold. It is not a treatment plan a clinician builds for you. It is a plan you own, informed by clinicians and people who know you well.
SAMHSA frames recovery as a self-directed process where you improve your health, live on your own terms, and work toward your version of a full life 8. Translate that into your map by writing three things down:
- What you want more of in the next year: sleep, unhurried mornings, real friendships, a specific project at work, time with your kids that isn't rushed.
- What specifically threatens those things: the 9 p.m. wine cue after the kids are asleep, the airport bar habit, the client dinner you keep saying yes to.
- The concrete supports and boundaries that make the first list possible and the second list less dangerous.
Your map has to survive contact with reality. If you travel two weeks a month, a plan built around a Tuesday 7 p.m. group is already broken. If your family visibility means group settings feel exposing, plan for individual sessions, telehealth check-ins, or a recovery companion who can meet you at a hotel instead. If your job runs on unpredictable evenings, your check-ins move to mornings and your accountability structure runs through text and phone rather than in-person meetings.
Write the map on one page. Date it. Share it with the two or three people who will actually help you keep it. Then plan to rewrite it at 30 days, when reality has done some editing of its own.
Scheduled Recovery Checkups Instead of Passive Discharge
Here is where most aftercare falls apart. You leave treatment, you get told to call if you need anything, and then nobody calls you. Passive discharge assumes you'll notice when something is off and reach out in time. That assumption is exactly backward. The moments you most need a check-in are the moments you're least likely to schedule one.
Scheduled recovery checkups flip the default. Instead of waiting for you to raise your hand, a clinician, coach, or care coordinator has standing appointments on the calendar—weekly at first, then every two weeks, then monthly, then quarterly as things stabilize. The checkup itself is short and structured. Somebody asks how you're actually doing, screens for warning signs you might be minimizing, adjusts your plan, and re-links you to services quickly if something is drifting.
The evidence for this is unusually clean for a behavioral intervention. A 2023 randomized trial embedded recovery management checkups in primary care and tracked participants over three months against a control group receiving standard care. Participants with scheduled checkups had more than twice as many days engaged in specialty treatment—14.45 days versus 7.13 days—and 41.3 days abstinent versus 31.9 days for the control group 2. That's a meaningful gap produced by nothing more sophisticated than someone reliably reaching out.
Over longer horizons, the pattern holds. Two clinical trials of quarterly recovery checkups tracked people for two years and found higher rates of returning to treatment when something slipped (60% versus 51% in one study, 55% versus 37% in the other) and a higher proportion of days abstinent (70% versus 63%) 3. The mechanism is not magic. It's that a scheduled contact catches a slip in week one instead of week six, when the cost of getting back on plan is much higher.
Build the checkup schedule into your calendar the same way you'd schedule anything you care about:
- For the first 30 days, weekly.
- For the next 60, every two weeks.
- From month three to month six, monthly.
- Past six months, quarterly, with the door open to increase frequency during high-risk windows—travel-heavy quarters, anniversaries, family stressors, career transitions.
If your current clinician doesn't offer this rhythm, ask for it explicitly or add a recovery coach or care coordinator who does.

Case Management as the Connective Tissue
You already know that recovery involves more than one appointment. There is the therapist, the psychiatrist if you have one, the primary care doctor, the coach, the group if you're in one, the family sessions, the labs, the prescription refills, the referrals when something new comes up. Case management is the person and process that keeps all of that connected so you don't become your own switchboard.
SAMHSA describes comprehensive case management as a client-centered process with five core functions: assessment, planning, linkage, monitoring, and advocacy 5, 6. In plain terms, someone maps what you need, builds the plan with you, gets you connected to the right services, checks that those services are actually working, and pushes back on the system when something is stuck. For a discreet, high-functioning reader, this often looks less like a caseworker at a clinic and more like a coordinator who takes calls at 6 a.m. before your flight, handles the paperwork you don't have time to chase, and makes the introductions that would otherwise take three weeks of phone tag.
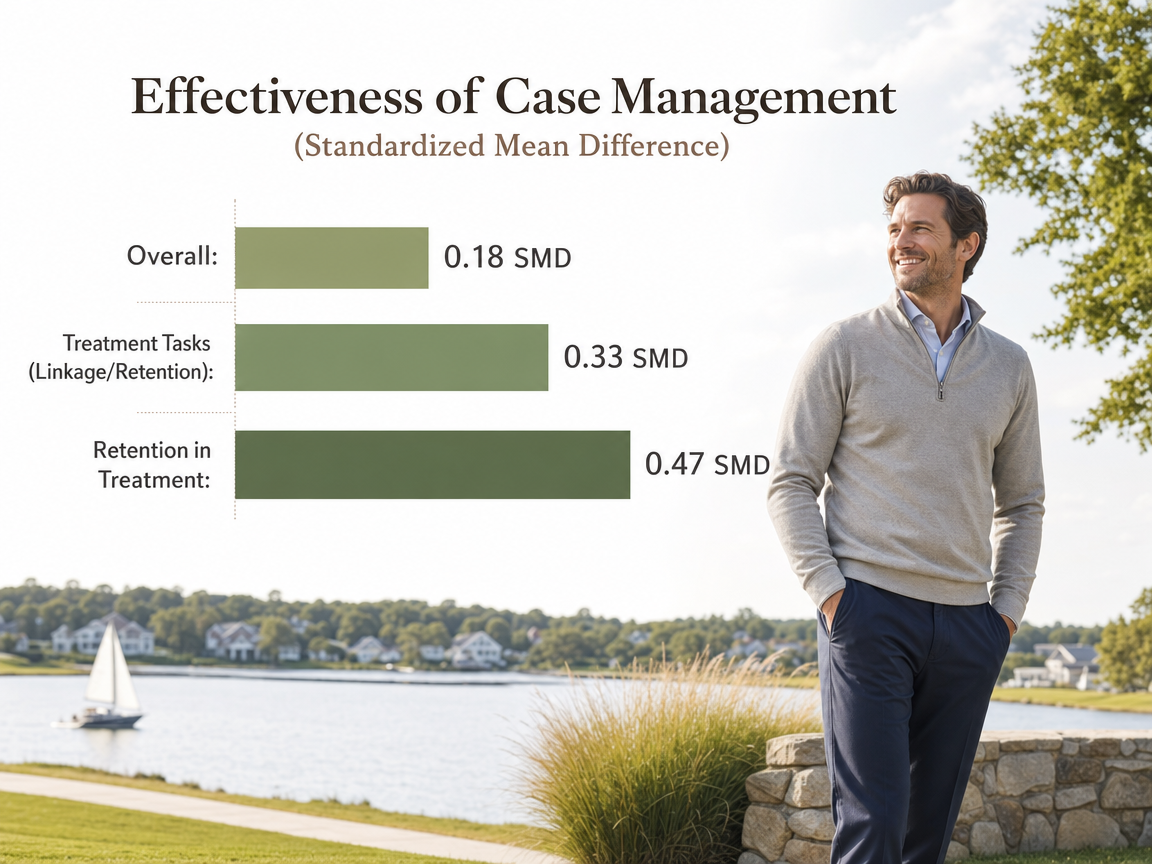
Be honest about what case management does and doesn't do. A meta-analysis of 21 randomized trials found that case management produced a small but statistically significant overall effect (SMD 0.18) compared to treatment as usual. The effect was larger for treatment-related tasks (SMD 0.33) and largest for retention in treatment (SMD 0.47). It was smaller—and not statistically significant—for direct changes in substance use or broader personal functioning 1. Read the shape of that carefully. Case management's superpower is keeping you engaged with the services that actually change behavior. It is the connective tissue, not the muscle.
That framing matters for what you should expect. A good case manager doesn't replace your therapist or run your recovery. They make sure you never lose a Tuesday because the referral fell through, that your medication doesn't run out mid-trip, and that when a new stressor lands—a parent's illness, a legal question, a housing decision—there is somebody whose job is to sort the logistics while you stay focused on the parts only you can do. Ask specifically who plays this role on your team. If nobody does, that gap is worth filling before you fill anything else.
A Written Crisis Protocol You Can Actually Use at 2 a.m.
A crisis protocol is not a hotline number scribbled on the fridge. It is a written document that tells a specific version of you—the version at 2 a.m. in a hotel room, or standing on the sidewalk outside a restaurant, or sitting in a parked car after an argument—exactly what to do next.
SAMHSA's 2025 crisis care guidelines describe what a coordinated response looks like: person-centered plans, clear roles, warm handoffs to ongoing services, and follow-up contacts after the moment passes 9. Translate that into your own document. It should name, in writing, three levels of contact:
- First-line: the two people you can call any hour without hesitation, ranked.
- Second-line: your clinician's after-hours line or a specific coach with 24-hour availability.
- Third-line: 988 for suicidal or urgent mental health crises, plus the nearest emergency department address if you need it in a rush.
Then it should list the four or five actions that come before any call. Leave the location. Go to a specific safer place you've pre-identified—your home, a friend's, a hotel lobby, a 24-hour café. Text a pre-written message to one of your first-line people. Delay any decision by one hour. Use a specific self-regulation practice you've actually rehearsed, not one you read about once.
Two details make this real. First, rehearse it. Read it out loud with the person on your first-line list so they know what happens when the text arrives. Second, write in a warm handoff after the crisis eases—who calls you the next morning, when your next checkup shifts to, whether the plan needs revision. A crisis without a follow-up is a plan that stops mid-sentence. The people who recover well have already answered the question of what Monday looks like before Sunday night gets hard.
A Relapse-Prevention Behavioral Routine
The last component is the one that runs every day, whether you feel like it or not. Call it a behavioral routine—the set of small, repeated actions that make relapse prevention a lived structure instead of an idea you agree with.
A well-known synthesis of relapse prevention research organizes it around five practical rules: change your life, be completely honest, ask for help, practice self-care, and don't bend the rules 15. Each one becomes a concrete behavior in your week, not a slogan:
- "Change your life" is the standing 6 a.m. workout that displaces the old evening habit and the removed contacts in your phone.
- "Be completely honest" is the weekly call where you say the thing you'd rather not say.
- "Ask for help" is the text you send before the craving peaks, not after.
- "Practice self-care" is a real sleep window, real meals, and time outside.
- "Don't bend the rules" is what you tell yourself when the trip to the client dinner feels manageable and you're negotiating with yourself about the second glass.
The Matrix intensive outpatient manual translates the same logic into daily-life behaviors that carry into aftercare: schedule your activities every day, avoid people who use substances, avoid known triggers when you can, pay obligations promptly so financial stress doesn't stack, and use specific techniques like thought-stopping when cravings arrive 4. None of these are dramatic. They're the boring architecture that makes everything else possible.
Build your routine on paper for the first 90 days:
- Morning anchor: what you do in the first hour before your phone owns you.
- Evening anchor: what you do in the last hour before bed.
- Weekly anchor: your check-in, your longest workout, your one real social contact with someone in recovery.
- Trigger response: the two or three moves you make when a craving lands.
Celebrate specifics as you build it. The first week you make it through a Wednesday check-in without rescheduling is a real signal. The first business trip where the evening looks nothing like it used to is a real signal. These are not small. They are the plan doing its job.
Insight Beyond Treatment
At Next Level Wellness & Behavioral Health, we believe meaningful change starts with perspective, not just protocols.
That philosophy is directly led by Amanda Marino, whose voice in behavioral health extends beyond clinical settings into leadership, culture, and personal growth.
Through keynote speaking and live events, Amanda explores the deeper themes that show up in recovery, family systems, and life transitions: authenticity, resilience, accountability, and the courage to change. Her work invites audiences to move past labels and into honest conversations that create lasting impact.
How the Plan Adapts Across 12 Months
A plan that looks the same in month one and month nine isn't a plan. It's a document. The evidence points toward continuing care lasting at least three to six months, with up to twelve months often necessary for durable recovery 11. What changes across that window is not whether you have a plan, but what the plan asks of you.
Day 1 to 30. Intensity is high on purpose. Weekly clinician contact, weekly recovery checkup, daily behavioral routine written on paper, first-line crisis contacts rehearsed out loud with the people on your list. Your recovery map is a working draft, not a finished document. Expect to rewrite it once during this month when reality corrects your assumptions.
Day 30 to 90. The map gets its first real edit. Checkup frequency moves to every two weeks. You start noticing which parts of the routine hold and which parts you keep skipping—that data matters. Case management shifts from setup to maintenance: refills running smoothly, referrals in place, the calendar working. If a business trip lands in this window, treat it as the first live test of the plan, not a threat to it.
Month 3 to 6. Monthly checkups. The behavioral routine should feel less like a script and more like your actual life. This is often when people quietly disengage because things are going well. Don't. The continuing-care evidence is specific here: the benefits of ongoing support get stronger over time, not weaker 10. Staying in the system is what compounds.
Month 6 to 12. Quarterly checkups with the door explicitly open to increase frequency during known high-risk windows—travel-heavy quarters, family anniversaries, career transitions, holidays. Your map gets a full rewrite around month nine. Ask what you want the next twelve months to look like now that you know what the last twelve actually did.
Where Group Work, Peer Support, and 12-Step Fit In
None of these modalities are the plan. They're options that live inside it. SAMHSA describes group therapy as an efficient format for building peer support and practicing coping skills after primary treatment 7—useful for some readers, wrong for others. If your family visibility or career means walking into a room of familiar faces is a real cost, that cost is legitimate. Discreet alternatives exist: private group formats, closed professional peer groups, telehealth cohorts, and one-to-one peer coaching all count as peer support.
Twelve-step involvement is one path, not the path. If it fits your beliefs and schedule, use it. If it doesn't, build peer connection another way—a weekly call with one person in recovery, a closed online community, or scheduled contact with a recovery coach. The plan needs peer contact. It does not need a specific room on a specific night.
Building the Plan This Week
You don't need a perfect plan by Sunday. You need a working one by Friday.
Open a blank page and write four things:
- Your one-page recovery map, in draft form.
- The names of the two people on your first-line crisis contact list, texted today so they know they're on it.
- The next four weeks of checkups already on your calendar, with times you'll actually keep.
- Your morning and evening anchors for the next seven days, specific enough that somebody else could read them and know what you're supposed to be doing at 7 a.m. Tuesday.
Then ask who is coordinating the rest. If nobody on your current team is holding the connective tissue—refills, referrals, the logistics that eat time you don't have—that gap is worth filling this week, not next month. A concierge case management arrangement, like the kind Next Level Wellness & Behavioral Health offers, exists precisely for readers whose lives don't fit a clinic schedule.
The plan gets stronger by getting written down and getting used. Start there.
Frequently Asked Questions
How long should an aftercare plan last?
Plan for at least 12 months, with 3 to 6 months as the absolute floor. Continuing-care research supports extending structured support up to a full year for durable recovery 11. What matters more than the end date is that the plan changes as you do, with checkup frequency, support intensity, and goals updated at 30 days, 90 days, and every quarter after.
What's the difference between a discharge plan and an aftercare plan?
A discharge plan is a snapshot of referrals and appointments handed to you the day you leave. An aftercare plan is an operating system that keeps working when reality shifts. It includes a written recovery map, scheduled checkups, case management for the connective tissue, a crisis protocol, and a daily behavioral routine. The discharge plan is one input into the aftercare plan, not a substitute for it.
Do I have to attend 12-step meetings for aftercare to work?
No. Twelve-step involvement is one option, not a requirement. Your plan needs consistent peer contact and structured support, but that can happen through private group formats, telehealth cohorts, closed professional peer groups, one-to-one recovery coaching, or scheduled calls with someone else in recovery 7. Choose the format that fits your schedule, privacy needs, and beliefs. The mechanism matters more than the room.
How often should recovery checkups happen?
Weekly for the first 30 days, every two weeks through day 90, monthly through month six, then quarterly. Increase frequency during high-risk windows like travel, anniversaries, or family stress. The evidence supports scheduled outreach over passive check-in: participants with structured recovery checkups had more than twice as many days in specialty treatment (14.45 vs 7.13) and more abstinent days over three months 2.
What should a written crisis protocol actually include?
Three tiers of contacts (two first-line people, an after-hours clinician or 24-hour coach, and 988 plus the nearest ER), a list of four or five actions to take before calling anyone, a pre-identified safer location, a rehearsed self-regulation practice, and a warm handoff for the morning after 9. Read it out loud with the people on your first-line list so nothing is theoretical.
Can aftercare planning stay private if my career or family visibility is a concern?
Yes. Discreet aftercare is a legitimate design choice, not a compromise. Individual sessions, telehealth check-ins, private peer cohorts, and concierge case management can replace open community meetings without weakening the plan. A recovery companion who meets you at a hotel or handles logistics before a flight keeps the structure intact while protecting your visibility. The plan needs consistency and peer contact, not a specific venue.
References
- A Meta-Analysis of the Efficacy of Case Management for Substance Use Disorders: A Recovery Perspective. https://pmc.ncbi.nlm.nih.gov/articles/PMC6477913/
- Using recovery management checkups for primary care to improve linkage to specialty substance use disorder treatment: A randomized trial. https://pubmed.ncbi.nlm.nih.gov/36208061/
- Quarterly Recovery Management Checkups to Treat Chronic Substance Use Disorders. https://www.bu.edu/aodhealth/2009/05/01/quarterly-recovery-management-checkups-to-treat-chronic-substance-use-disorders/
- Counselor's Treatment Manual: Matrix Intensive Outpatient Treatment for People With Stimulant Use Disorders. https://library.samhsa.gov/sites/default/files/sma13-4152.pdf
- Comprehensive Case Management for Substance Use Disorders. https://library.samhsa.gov/sites/default/files/PEP20-02-02-013.pdf
- TIP 27: Comprehensive Case Management for Substance Abuse Treatment. https://library.samhsa.gov/sites/default/files/sma15-4215.pdf
- Substance Abuse Treatment: Group Therapy. https://library.samhsa.gov/sites/default/files/sma15-4024.pdf
- Recovery and Support. https://www.samhsa.gov/substance-use/recovery
- 2025 National Guidelines for a Behavioral Health Coordinated System of Crisis Care. https://library.samhsa.gov/sites/default/files/national-guidelines-crisis-care-pep24-01-037.pdf
- How effective is continuing care for substance use disorders? A meta-analytic review. https://pmc.ncbi.nlm.nih.gov/articles/PMC3840113/
- The Continuing Care Model of Substance Use Treatment: What Works, and When Is “Enough,” “Enough?”. https://pmc.ncbi.nlm.nih.gov/articles/PMC4007701/
- Impact of Continuing Care on Recovery From Substance Use Disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC7813220/
- Recovery Management Checkups: A Future Function of Addiction Treatment?. https://pmc.ncbi.nlm.nih.gov/articles/PMC6329465/
- Continuing Care Research: What We’ve Learned and Where We’re Going. https://pmc.ncbi.nlm.nih.gov/articles/PMC2670779/
- Relapse Prevention and the Five Rules of Recovery. https://pmc.ncbi.nlm.nih.gov/articles/PMC4553654/
A Voice Shaping the Conversation
The topics explored here—change, self-awareness, recovery, and growth—are the same themes Amanda Marino brings to audiences nationwide through speaking engagements and live events.
Known for her appearances on A&E’s Intervention and Digital Addiction, Amanda speaks to organizations, communities, and leadership teams about navigating adversity, embracing vulnerability, and building lives rooted in purpose. Her message resonates far beyond treatment, offering insight that applies to families, professionals, and anyone standing at a crossroads.



Heal on your terms—any time, anywhere.