
How Failure to Launch Treatment Helps Your Family

Key Takeaways
- Structured family-based treatment shifts the household within weeks, with parents sleeping better and the adult child showing small, concrete gains in daily rhythm before larger changes follow.
- Willpower conversations fail because anxiety, avoidance, and parental accommodation form a reinforcing loop; the real intervention is coached reduction of accommodations, not more motivation talks 10.
- Family-based treatment targets four measurable domains, employment, living arrangements, social behavior, and engagement with the adult world, transferred gradually so gains hold under pressure 1.
- Parents can start treatment alone when an adult child refuses to participate, using a clinician-guided parent-only track that has produced functional gains even without the young adult in sessions 10.
What Actually Changes at Home in the First 90 Days
You already know the shape of your days. The closed bedroom door. The dishes that appear at 2 a.m. The careful way you time your questions so the conversation doesn't end before it starts. If you're reading this, you're not looking for a definition of failure to launch. You're looking for what actually shifts when a family gets real help.
In the first 90 days of structured treatment, the change you notice first isn't your adult child. It's you. Parents who begin a family-based track usually stop carrying the whole weight of the household emotional temperature within the first few weeks. You start sleeping through the night. You stop rehearsing the next difficult conversation in the shower.
Then the household rhythm shifts. Small, concrete things: a scheduled wake-up that holds three days in a row. A resumed text thread with an old friend. One completed job application, not five promised ones. Clinicians who work with highly dependent young adults describe gains in employment, living arrangements, social behavior, and engagement with the adult world after structured family-based intervention 1. Those gains rarely land all at once. They arrive in fragments you can point to.
What also changes is the argument. When a professional is coordinating the plan, you stop being the person who has to name every expectation and enforce every consequence. That single shift, moving from lone enforcer to supported parent, is often what makes the next 90 days possible.
The Dependency Trap: Why Willpower Talks Haven't Worked
Anxiety, Avoidance, and Accommodation as a Loop
You've probably had the willpower talk more times than you can count. The one where you sit down calmly, name what needs to change, and get either agreement or silence. And then nothing shifts. If that pattern has repeated for a year or more, the problem isn't your delivery. It's that willpower isn't what's driving the stuckness.
Clinical work with highly dependent young adults describes something more specific: a dependency trap in which anxiety, avoidance, and family accommodation feed each other. Your adult child feels overwhelmed by an adult task, whether that's a phone call, a class registration, or a job application. Avoiding it brings immediate relief. You, seeing the distress, step in, smooth it over, or take the task off their plate. The relief teaches the nervous system that avoidance works, and the next challenge feels even bigger. As Lebowitz puts it, the young adult"relies on parents for help in avoiding challenges that feel insurmountable, and the parental accommodations reinforce the avoidance and lack of self-efficacy"10.
Read that once more, slowly. The loop is not about laziness. It's about a threat response that has been rehearsed thousands of times.
This is why willpower talks don't work. You're asking your adult child to override a loop that also runs through you. The intervention point isn't more motivation. It's a structured, coached reduction of the accommodations that keep the loop spinning, done in a way that protects the relationship rather than blowing it up 10. That's the reframe that changes everything about what to try next: you stop trying to talk your child into a different mindset and start changing the conditions that made avoidance the easier option. It's a slower entry, but it's the one that actually holds.
How Earlier Family Patterns Set the Stage (Without Blame)
Here's the part parents brace for, so let's take the sting out of it up front: understanding how you got here is not the same as being blamed for it. You were parenting a specific child, in specific circumstances, with the information you had. Most parents who end up in a failure to launch situation were doing what looked like careful, loving work at the time.
Still, the research is worth knowing. A 2022 study of autonomy-restricting parenting found that controlling behaviors used in early adolescence were more strongly linked to parental dependence in emerging adulthood than the same behaviors used later, and that accommodation patterns correlated with lower distress tolerance and higher anxiety and rumination in young adults 5. Translation: when kids are shielded from age-appropriate friction early on, the muscle for tolerating hard feelings doesn't fully develop.
Notice what that gives you. Not guilt. Leverage. If accommodation patterns can be learned, they can be unlearned, on both sides. A good clinician won't ask you to catalog every choice you wish you'd made differently. They'll ask what you're accommodating right now, this week, and help you decide which one to change first. That's a working plan, not a verdict on your parenting.
What Structured Treatment Looks Like When It Works
Assessment First: Anxiety, Depression, Substance Use, or All Three
Before anyone hands you a plan, a good clinician spends real time figuring out what you're actually dealing with. That matters because failure to launch is not a diagnosis. It's a pattern that sits on top of other things, and the mix under the surface changes what treatment should target first.
A careful assessment typically looks at four overlapping layers:
- anxiety and avoidance patterns
- depressive symptoms
- any substance use
- the specific accommodations happening at home
The Lebowitz literature is direct about why labels alone don't cut it, arguing for careful assessment over reliance on the failure to launch shorthand, since the underlying drivers vary from one young adult to the next 1.
The substance use question deserves its own honest look. Research on emerging adults with serious mental health conditions found that substance use in this age group is common and linked to poorer employment and educational outcomes 4. If you've wondered whether what you're seeing is anxiety, low motivation, cannabis use, or all three quietly feeding each other, you're asking the right question. A skilled assessor will ask it too, without judgment, and design the plan around the actual answer.
What you should walk away with after assessment: a short written picture of what's driving the stuckness, a first target that's specific enough to act on this week, and a clear sense of who is doing what. If you leave the intake with only a diagnosis and a schedule, ask for more.
The Four Domains That Improve After Family-Based Treatment
Parents often ask, understandably, what "better" is supposed to look like. Not in feelings, which are harder to measure, but in the visible parts of a life. The clinical literature on failure to launch gives a surprisingly concrete answer.
In the Lebowitz work with highly dependent adult children, families who completed structured, family-based intervention saw gains across four specific domains: employment, living arrangements, social behavior, and other forms of engagement with the adult world 1. That's the scope worth holding in mind. It's a clinical case series describing young adults who were highly dependent on their families, not a population-level randomized trial. Still, those four domains are useful because they map onto what you actually see at the kitchen table.
Here's what that can look like in practice, one domain at a time.
- Employment.
- Not a career leap. A first part-time shift held for a month. A completed application without three prompts. A conversation about money that doesn't end in a door closing.
- Living arrangements.
- A move from parents' bedroom-across-the-hall to a converted basement space with its own rhythm. Later, sometimes, a roommate situation or supported housing. The direction matters more than the speed.
- Social behavior.
- A resumed friendship. A weekly plan outside the house. A group therapy connection that becomes a text thread.
- Engagement with the adult world.
- Handling their own doctor's appointment. Renewing an ID. Voting. Calling the pharmacy without you on speaker.
You will not get all four at once, and you won't get them in a straight line. But when treatment is working, you can name which domain moved this month, and that becomes the metric your family runs on.

The Gradual Transfer of Responsibility
The word that keeps coming up in good treatment plans is gradual. Not because clinicians are cautious by temperament, but because sudden handoffs tend to fail in ways that set families back months.
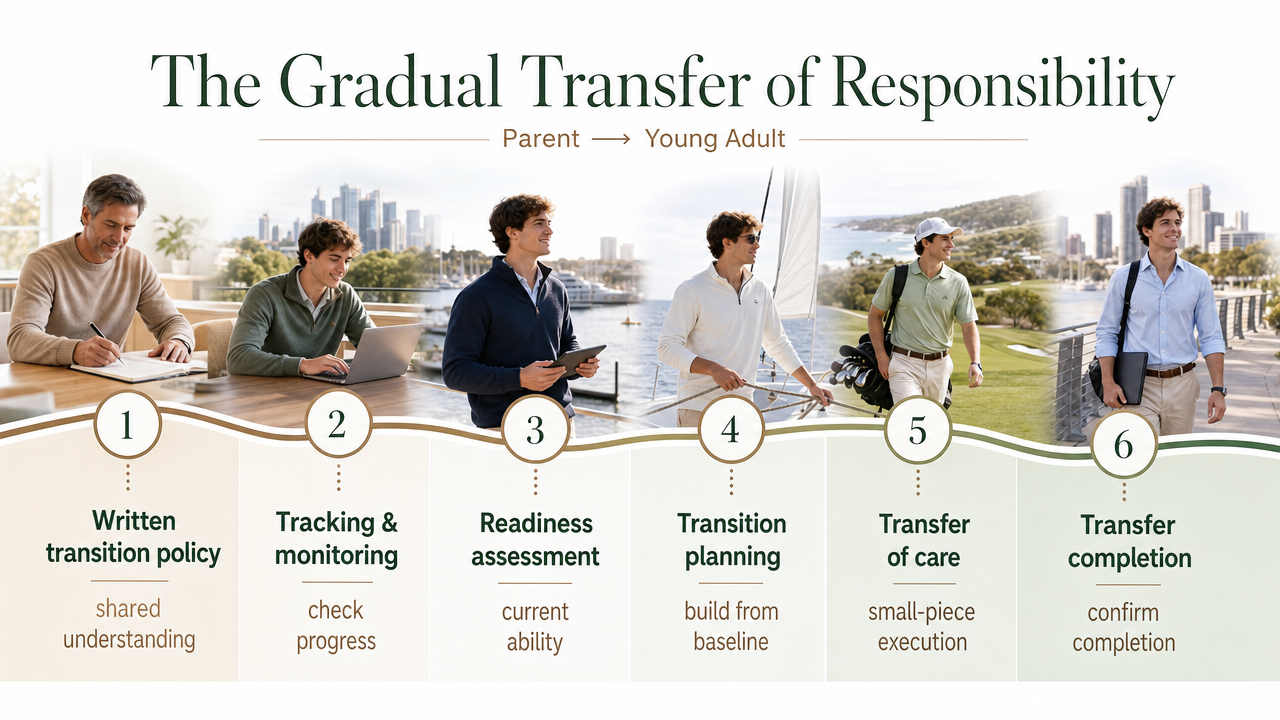
A useful frame comes from the youth health transition literature, where responsibility for medical care is deliberately shifted from parent to young adult across six core elements:
- a written transition policy
- tracking and monitoring
- readiness assessment
- transition planning
- transfer of care
- transfer completion 6
That framework was built for pediatric-to-adult healthcare, but the logic translates well to behavioral health and independence work. You start with a shared understanding of what's changing, check what your adult child can actually handle right now, build the plan around that baseline, execute in small pieces, and confirm that each piece has landed before adding the next.
In a failure to launch context, that might look like this. Month one: a written agreement about what the household expects and what the parents will stop absorbing. Month two: a readiness check on a specific skill, say, managing a weekly medication refill. Month three: your adult child owns that refill fully, and you formally hand off the next task. The gradual transfer of responsibility framework isn't a promise of speed. It's a promise that each transfer will be planned, practiced, and confirmed, so gains don't collapse the first time something gets hard. That's the difference between forward motion and the same argument in a new month.
Insight Beyond Treatment
At Next Level Wellness & Behavioral Health, we believe meaningful change starts with perspective, not just protocols.
That philosophy is directly led by Amanda Marino, whose voice in behavioral health extends beyond clinical settings into leadership, culture, and personal growth.
Through keynote speaking and live events, Amanda explores the deeper themes that show up in recovery, family systems, and life transitions: authenticity, resilience, accountability, and the courage to change. Her work invites audiences to move past labels and into honest conversations that create lasting impact.
The Parent-Only Track Is a Legitimate Starting Point
The parent-based model developed for highly dependent young adults was designed for exactly this situation. Parents work with a clinician to systematically reduce accommodations, hold ground without escalation, and change what the household actually rewards, all without requiring the young adult to sit in a therapy office 10. It's not a workaround. It's the intervention. And the Lebowitz work reports meaningful functional gains for the young adult even when the parents were the ones doing the clinical work 10.
What this looks like in practice: you meet with a clinician weekly, sometimes with your co-parent, sometimes alone. You map the accommodations that are currently in place, meals delivered to the bedroom door, bills silently paid, appointments made on their behalf, and choose one or two to change first. You script how you'll communicate the change with warmth, not ultimatum. You plan for the pushback, because there will be pushback. Then you hold the change, supported, while your clinician helps you read what happens next.
SAMHSA's family counseling guidance backs the underlying logic: family systems work can shift communication patterns and reduce enabling dynamics that keep a loved one stuck, and it works even when the person of concern isn't yet engaged in their own treatment 8.
A few things worth naming. The parent-only track is not a punishment strategy. It's not tough love repackaged. And it's not you doing therapy on your child by proxy. It's you getting coached on the specific behaviors that have been maintaining the loop, so those behaviors can change in a way that's steady and kind. Often, once parents make visible shifts and stop absorbing the anxiety of every adult task, the young adult's own willingness to engage in treatment changes too. Not always. But often enough that starting alone is a real path forward, not a consolation prize.
When Substance Use Is Part of the Picture
Many parents arrive at this question sideways. You didn't set out to ask whether your adult child has a substance use problem. You noticed the sleep schedule, the flat affect, the smell in the hallway, the way certain conversations end. And you've quietly wondered whether what looks like avoidance is also something being medicated.
You're not wrong to ask. Substance use among emerging adults with serious mental health conditions is common enough that it needs to be part of any honest failure to launch assessment, and it is linked to poorer employment and independence outcomes when it goes unaddressed 4. That's not a reason to lead with alarm. It's a reason to make sure the plan you're building actually treats what's there, not just what's easiest to see.
Integrated care matters here. When anxiety, low mood, and substance use are running together, treating one and ignoring the others tends to produce short gains that don't hold. SAMHSA's family counseling guidance describes how family systems work can shift communication patterns and reduce enabling dynamics in substance use contexts, which is often the missing piece when parents have tried individual therapy referrals that didn't stick 8. The family, in other words, is part of the treatment, not a spectator to it.
A practical note: you don't need a confirmed diagnosis before starting. A skilled clinician can hold the substance use question open during assessment and adjust the plan as the picture clarifies. What you're looking for is a team that won't force a false choice between mental health treatment and substance use treatment. Your adult child likely needs both, coordinated, at the same pace.
What Your Adult Child Experiences as Supportive vs. Pressuring
One thing parents rarely get to hear: what the same conversation sounds like from the other side of the table. And it matters, because the difference between a comment that helps and one that shuts things down is often smaller than you'd think.
Qualitative work with emerging adults describes how family stress shapes self-concept, coping, and interpersonal relationships during this stage, and the researchers caution that what feels supportive to one young adult may feel stressful to another 3. That's a useful piece of humility to carry into your next conversation. There is no universal script.
Still, some patterns hold. Young adults tend to experience these as supportive:
- specific, time-bound offers ("I'm driving past the pharmacy at 4, want me to grab your refill this once?")
- curiosity without a follow-up quiz
- consequences that were named in advance and applied without a lecture
They tend to experience these as pressuring:
- broad questions about the future asked in passing
- comparisons to siblings or cousins
- help that arrives with visible sighs
The practical move is to ask your clinician to help you script two or three recurring conversations, the morning check-in, the money conversation, the weekend plan question, in language your adult child can actually hear. Small wording shifts, coached and practiced, change what your child walks away believing about your intentions.
Aftercare Is Where Families Actually Feel Relief
Here's the part parents don't hear enough about. The structured phase of treatment, the weekly clinical meetings, the accommodation maps, the scripted conversations, is not where families exhale. That comes later, in the aftercare phase, when the plan you built starts running on its own steam.
The research on young adults with substance use disorders is clear on why this phase matters. Evidence-based reviews argue that this age group needs access to a broad range of interventions and continuing care to sustain the gains from early treatment 7. Continuing care is not a nice-to-have layer. It's the reason the first three months don't quietly unwind by month six. For families where mental health and substance use both showed up in the assessment, aftercare is where the two threads stay stitched together instead of drifting apart.
What relief actually feels like: a clinician who still checks in monthly instead of weekly. A written plan for what happens if your adult child misses two shifts in a row or stops taking a medication. A short list of the accommodations you agreed not to resume, taped somewhere you can see it when the pull to smooth things over gets strong. SAMHSA's family therapy guidance emphasizes that ongoing family involvement helps sustain adherence and reduces relapse risk over time, which is another way of saying the family stays part of the plan, just at a lighter cadence 2.
You'll notice the household changes too. The house gets quieter in a good way. You stop bracing for the next crisis because the plan already names what happens if one arrives. That is what relief sounds like: not the absence of hard days, but the presence of a system that holds when they come.
A Direct Word to Parents Deciding What to Do Next
You have already been doing hard work for a long time. What you need now isn't more resolve. It's a plan with someone else's hand on it.
A reasonable next step is short. Book one assessment with a clinician who understands the dependency trap and can hold the substance use question open without flinching. Ask them how they'd structure the first 30 days, whether your adult child engages or not. Listen for specifics, not slogans.
If you're not sure where to start, SAMHSA's National Helpline is free, confidential, and available 24/7 for treatment referrals and information 9. For families wanting concierge-style coordination that adapts to your schedule and privacy, Next Level Wellness & Behavioral Health builds plans around exactly this situation.
Frequently Asked Questions
How long does failure to launch treatment usually take?
There's no fixed timeline, and any clinician who promises one is guessing. Most families see the first concrete shifts in household patterns within 8 to 12 weeks of structured work, with meaningful functional gains developing over 6 to 12 months. Continuing care matters more than program length. Young adults with substance use or mental health challenges benefit from ongoing support to sustain early gains rather than a hard stop at graduation 7.
Can treatment work if my adult child refuses to participate?
Yes. The parent-based model was designed for exactly this scenario. You work with a clinician to systematically reduce accommodations and change what the household reinforces, without requiring your adult child to attend sessions. Reported outcomes include functional gains for the young adult even when parents did the clinical work 10. Often, once the accommodation patterns shift at home, your adult child's own willingness to engage changes too.
How do we tell the difference between failure to launch, depression, and a substance use problem?
You don't have to. That's the assessment's job. Failure to launch is a pattern, not a diagnosis, and it often overlaps with anxiety, depression, and substance use rather than replacing them. Substance use among emerging adults with serious mental health conditions is common and linked to poorer employment and independence outcomes 4. A good clinician holds all three questions open at once and designs a plan around what's actually there.
Are we making things worse by letting our adult child live at home?
Living at home is not the problem. The specific accommodations that quietly do adult tasks for your adult child are what maintain the loop. Research links parental accommodation patterns to lower distress tolerance and higher anxiety in emerging adults 5. The fix isn't moving your child out. It's identifying which accommodations to change, in what order, with clinical support, so your home becomes a place where independence can actually grow.
What does the parent-only track actually involve?
You meet weekly with a clinician, often with your co-parent. You map current accommodations, choose one or two to change first, and script how you'll communicate the change without ultimatum. You plan for pushback, then hold the change with support. SAMHSA's family counseling guidance backs the logic: family systems work can shift communication and reduce enabling patterns even when the person of concern isn't yet engaged in their own treatment 8.
What happens after the structured phase of treatment ends?
Aftercare is where families exhale. Clinical check-ins move from weekly to monthly, and you keep a written plan for what happens if things wobble. SAMHSA notes that ongoing family involvement helps sustain treatment adherence and reduces relapse risk over time 2. You'll still have hard days. The difference is that the plan already names what to do when one arrives, so you're no longer improvising in the middle of a crisis.
References
- “Failure to Launch”: Shaping Intervention for Highly Dependent Adult Children. https://pmc.ncbi.nlm.nih.gov/articles/PMC4895190/
- Family Therapy Can Help: For People in Recovery From Mental Illness or Addiction. https://library.samhsa.gov/product/family-therapy-can-help-people-recovery-mental-illness-or-addiction/sma15-4784
- Emerging Adults' Lived Experience of Formative Family Stress. https://pmc.ncbi.nlm.nih.gov/articles/PMC3964850/
- Prevalence and Impact of Substance Use among Emerging Adults with Serious Mental Health Conditions. https://pmc.ncbi.nlm.nih.gov/articles/PMC3767039/
- Parental Autonomy Restricting Behaviors During Adolescence as Predictors of Dependence in Emerging Adulthood. https://pmc.ncbi.nlm.nih.gov/articles/PMC9837864/
- Youth Health Transition Toolkit. https://ldh.la.gov/page/youth-health-transition-toolkit
- Evidence-Based Treatment for Young Adults with Substance Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC7879425/
- Chapter 3—Family Counseling Approaches. https://www.ncbi.nlm.nih.gov/books/NBK571088/
- National Helpline. https://www.samhsa.gov/find-help/helplines/national-helpline
- "Failure to Launch": Shaping Intervention for Highly Dependent Adult Children. https://pmc.ncbi.nlm.nih.gov/articles/PMC5504878/
A Voice Shaping the Conversation
The topics explored here—change, self-awareness, recovery, and growth—are the same themes Amanda Marino brings to audiences nationwide through speaking engagements and live events.
Known for her appearances on A&E’s Intervention and Digital Addiction, Amanda speaks to organizations, communities, and leadership teams about navigating adversity, embracing vulnerability, and building lives rooted in purpose. Her message resonates far beyond treatment, offering insight that applies to families, professionals, and anyone standing at a crossroads.



Heal on your terms—any time, anywhere.