
Getting Help Staying Sober After Rehab: A Guide

Key Takeaways
- The weeks following residential discharge carry substantial relapse risk, so treat this window as a transition in care rather than the end of treatment.
- Design a continuing care plan by combining outpatient therapy, peer coaching, mutual-help groups, medication, housing, and case management to fit your life.
- Stay actively engaged for at least three months, since NIDA identifies that threshold as when most people see meaningful improvement.
- Step down through the ASAM continuum from residential to IOP to outpatient, keeping medications for opioid or alcohol use disorder continuous.
- Choose peer coaching and mutual-help formats based on fit and consistent attendance, sampling several groups before committing to one rhythm.
- Audit your home environment on day one and structure the first 90 days in phases: stabilize, build cadence, then refresh the plan.
- Define family roles around check-ins and logistics rather than clinical details, protecting privacy while letting loved ones support recovery effectively.
- Treat a slip as information, not failure: contact your team the same day, keep medications going, and briefly escalate support.
Why the weeks after discharge decide the next year
The morning you leave residential treatment, the structured schedule that supported you for weeks or months disappears. Your phone reactivates, and the constant presence of support staff fades. The life you paused—work, family, and social engagements—resumes, creating a disorienting shift.
This period immediately following discharge is a particularly vulnerable time. A 2025 review of adults transitioning from non-hospital residential programs for opioid use disorder highlighted a substantial risk of relapse in the weeks after leaving. The authors emphasized that effective transition planning, continued medication management, and ongoing psychosocial support are crucial for positive outcomes. This pattern is consistent across various substance use challenges. Leaving treatment is not the end of the recovery journey; it is simply a change in its form.
The encouraging news is that sustained recovery through the first year is rarely achieved through sheer willpower alone. It is built on a foundation of structure. Decades of research on continuing care consistently show that longer, flexible, and actively engaged follow-up leads to better outcomes than a simple handoff with a phone number. Your goal in the coming weeks is not to struggle through but to construct a personalized plan that fits your schedule, respects your privacy, and connects you with the right support at the right times. This guide will help you navigate that process.
Build a continuing care plan, not a checklist
What continuing care actually means
Continuing care is far more than a pamphlet received at discharge. It represents a coordinated system of ongoing services designed to maintain your connection to treatment after the intensive phase concludes. View it not as a graduation, but as an evolution of your treatment format. The clinical work persists, but its delivery adapts to your life.
The National Institute on Drug Abuse (NIDA) frames recovery from a substance use condition as a gradual process requiring sustained medical, psychological, and social support, much like managing any chronic health issue. This perspective is vital because it alleviates the pressure to be "done" with treatment. Needing care in month six is not a setback; it aligns with evidence-based practices for long-term well-being.
A systematic review of continuing care studies revealed that over half of the trials reported significant improvements in substance use outcomes. The most robust results were observed in programs that extended over longer durations and proactively engaged individuals, rather than passively waiting for them to seek help. The key takeaway is clear: a passive approach—simply having a number to call in a crisis—is not an effective plan. A robust plan includes scheduled appointments, dedicated support individuals, and a consistent rhythm of engagement.
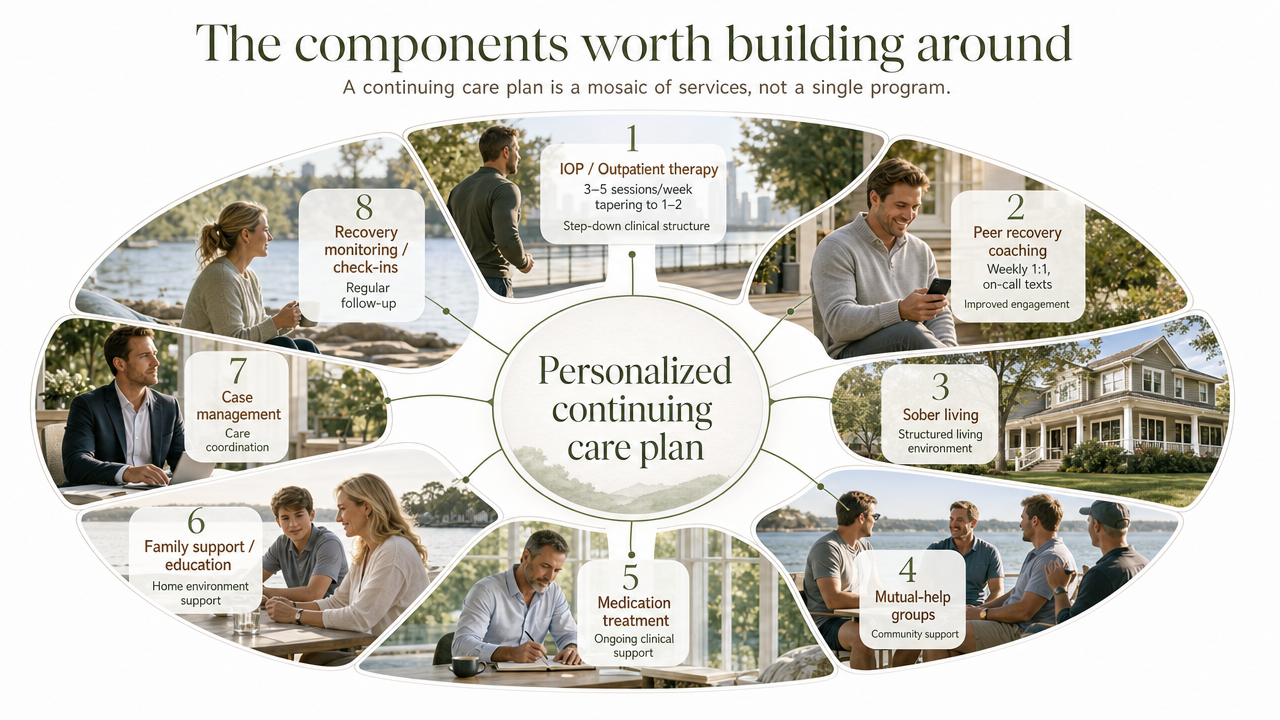
The components worth building around
A continuing care plan is a mosaic of different services, not a single program. Each component serves a distinct purpose and has been independently studied. Your task is to select the elements that best suit your lifestyle and arrange them to create a comprehensive support system.
The following table outlines the main components, drawing on resources such as ASAM's continuum of care, continuing care research, sober living outcomes literature, peer recovery services reviews, mutual-help comparison studies, NIDA's treatment guidance, and SAMHSA's case management advisories.
| Component | Typical cadence | Primary evidence | Best-fit scenario |
|---|---|---|---|
| IOP / Outpatient therapy | 3-5 sessions/week tapering to 1-2 | ASAM continuum 13 | Step-down from residential; clinical structure still needed |
| Peer recovery coaching | Weekly 1:1, on-call texts | Improved engagement and use outcomes 6 | You want a real person between clinical visits |
| Mutual-help groups | 1-5 meetings/week | Effective and free; match to preference 10 | You want community that outlasts any program |
| Recovery housing | 3-12 months residence | Improved use, employment, symptoms 5 | Home environment is unstable or high-cue |
| Medications for SUD | Daily/monthly per prescriber | Foundational for OUD/AUD 14 | Opioid or alcohol use disorder; craving management |
| Case management | Weekly to biweekly touch | Keeps people in care by removing barriers 16 | Complex logistics: travel, custody, medical, work |
| Digital tools | Daily self-guided use | Discreet supplemental support (studied) 7 | Between-session skills and privacy needs |
| Family involvement | Monthly to weekly check-ins | Families as resource when engaged well 8 | Loved ones are safe and want to help |
You do not need every option listed. The goal is to identify the right combination for your immediate 90-day plan, with the flexibility to adapt as your needs evolve.
The three-month engagement threshold and why it matters
If there is one critical metric to remember from this guide, it is the three-month engagement threshold. NIDA's training principles indicate that approximately three months of continuous engagement in treatment is the point at which most individuals experience significant improvement. The guidance emphasizes that no single treatment approach suits everyone and that plans should be updated as needs change. This three-month period is not a finish line, but rather a foundational minimum.
For someone transitioning from residential care, this often translates to:
- Consistent participation in an Intensive Outpatient Program (IOP) or outpatient therapy
- Regular check-ins with a peer coach or clinician between sessions
- Consistent engagement with at least one form of community connection, even when motivation wanes
The purpose of this threshold is not to achieve perfection, but to ensure sustained engagement.
Insight Beyond Treatment
At Next Level Wellness & Behavioral Health, we believe meaningful change starts with perspective, not just protocols.
That philosophy is directly led by Amanda Marino, whose voice in behavioral health extends beyond clinical settings into leadership, culture, and personal growth.
Through keynote speaking and live events, Amanda explores the deeper themes that show up in recovery, family systems, and life transitions: authenticity, resilience, accountability, and the courage to change. Her work invites audiences to move past labels and into honest conversations that create lasting impact.
Stepping down through the ASAM continuum
From residential to IOP to outpatient
The American Society of Addiction Medicine (ASAM) outlines a continuum of care, not an abrupt transition. ASAM categorizes care into five primary levels:
- Early intervention (Level 0.5)
- Outpatient (Level 1)
- Intensive outpatient (Level 2.1)
- Residential (Level 3)
- Medically managed intensive inpatient (Level 4)
When you complete a residential program, you are not left without support; you are moving down a structured ladder designed to maintain your connection to care as the intensity decreases.
A typical progression involves transitioning from Level 3 residential care to an Intensive Outpatient Program (IOP) at Level 2.1. This usually entails three to five clinical sessions per week for six to twelve weeks, incorporating group therapy, individual sessions, and sometimes family involvement. Following IOP, the next step is often Level 1 outpatient care, which might include weekly individual therapy combined with a consistent schedule of mutual-help meetings. Community supports like peer coaching, recovery housing, and digital tools complement these clinical levels rather than replacing them.
What truly matters is maintaining continuity within this system. Bypassing the intermediate steps and going directly from residential care to a "call if I need something" approach often leads to breakdowns in the recovery plan. If your discharge plan does not specify a particular IOP or outpatient team with a confirmed start date, it is crucial to request this information before leaving the facility.
Medications for substance use disorders
If you began medication for opioid or alcohol use disorder during residential care, ensuring the continuity of that prescription is paramount in your first week home. NIDA clearly states that addiction is a treatable condition and that medications are fundamental for opioid, alcohol, and nicotine use disorders. These medications are most effective when integrated with counseling or behavioral therapy. This approach is not a temporary measure but often forms the bedrock of sustained recovery for many individuals.
When you attend your first outpatient appointment, consider asking three key questions:
- Who will manage your prescriptions moving forward, and what is the refill process, especially when traveling?
- What is the plan if cravings intensify or if side effects interfere with your daily life?
- How will coordination occur between your prescriber and therapist to ensure seamless care, preventing you from having to relay information between them?
If you have a history of opioid or alcohol use and were not offered medication, it is appropriate to inquire directly about this. Ask for the rationale and what circumstances might lead to its consideration.
Contingency management as reinforcement
Contingency management (CM) is a highly researched yet often underutilized tool in recovery care. It involves providing small, structured incentives to reinforce positive behaviors, such as attending sessions, submitting negative drug screens, or actively engaging in treatment. A 2025 SAMHSA advisory describes CM as"a proven health care intervention with demonstrated effectiveness in treating a variety of substance use disorders"across diverse populations. It also clarifies how programs can implement CM using federal funds while adhering to specific compliance guidelines.
For some, CM might seem counterintuitive, as the motivation is not about the monetary value of a gift card. The underlying mechanism is behavioral, designed to make desired actions visible and reinforce them on a schedule that the brain can register. If your outpatient program incorporates a CM component, it is beneficial to engage with it seriously. If not, inquire whether such a program is available in your area.
Peer support, mutual-help groups, and choosing your fit
Recovery coaching and peer specialists
A recovery coach is distinct from a therapist or a sponsor, and this distinction is crucial. A trained peer specialist has personal experience with substance use challenges and is certified to support others on their journey. This support typically involves weekly one-to-one contact, on-call texting between clinical appointments, and practical assistance with logistical details that clinical sessions may not cover. A 2025 systematic review of peer recovery support services indicated that these services are linked to improved substance use outcomes, increased treatment engagement, and enhanced recovery-related functioning across multiple studies. While acknowledging variations in study designs, the authors noted the need for more rigorous trials.
For individuals in demanding professions, the unique nature of the coach-client relationship is often highly valued. Your coach can be the person you text before an important meeting, the one who meets you for coffee after a challenging weekend, or someone who knows where to find quiet spaces in an airport. When considering a coach, inquire about their certification, confidentiality practices, and how they manage communication, especially when you are traveling. A reasonable starting point is one weekly call combined with responsive texting.
12-step, SMART Recovery, and other mutual-help formats
Mutual-help groups are among the most cost-effective and enduring components of a continuing care plan. They also tend to evoke strong opinions. Alcoholics Anonymous and other 12-step fellowships have decades of supporting evidence and are recognized in peer-reviewed literature as an effective, free, and widely accessible source of support for individuals addressing alcohol use challenges. Alternatives such as SMART Recovery, LifeRing, and Refuge Recovery offer different frameworks, some secular, some based on cognitive-behavioral tools, and others rooted in mindfulness. Comparative research suggests that matching individuals to the group type they prefer is key, as sustained attendance is what drives positive outcomes.
It is advisable to sample different groups before committing. In your first month, try three or four meetings across two different formats. Observe the demographics of the attendees, whether the format allows for participation without requiring you to disclose your name or profession, and if you can consistently attend given your travel schedule. Online meetings and early-morning meetings are valuable options. A consistent Thursday 7 a.m. Zoom meeting that you never miss will likely be more beneficial than an in-person meeting you attend sporadically.
You are not obligated to choose one format and stick with it indefinitely. Many individuals create a hybrid approach, attending one 12-step meeting weekly for community and another SMART or specialty meeting for skill-building. The consistency of your attendance, rather than the specific label of the group, is what truly matters.
Environment, housing, and the first 90 days
The initial 90 days after discharge are less about monumental efforts and more about the subtle yet powerful influence of your immediate surroundings: the room you wake up in, your digital calendar, and the individuals who are aware of your well-being on a Sunday evening. Your environment plays a significant, often quiet, role. If elements that trigger past behaviors remain—such as a bar cart, active group chats with individuals still engaging in substance use, or old prescriptions in the medicine cabinet—your plan may be compromised before your first outpatient session.
Begin by conducting a thorough review of your home environment on the day you return. Remove anything that needs to be eliminated and make practical changes without unnecessary drama. If your home environment is unstable, presents high-risk cues, or is shared with individuals who are still using substances, recovery housing warrants serious consideration. A long-running study found that residents of sober living houses demonstrated improvements in substance use, employment, arrests, and psychiatric symptoms over time. A three-to-six-month stay in such housing should not be viewed as a step backward; for some, it can be the critical factor between a successful plan and one that falters.
The first 90 days can be structured into three phases, informed by aftercare planning research and NIDA's identified three-month engagement threshold for significant improvement:
Weeks 1-2: Stabilize the container. Confirm your outpatient team, first appointment, and medication continuity. Conduct an environmental audit of your home. Select your initial mutual-help meeting. Inform two trusted individuals about your Sunday-night check-in plan.
Weeks 3-6: Build cadence. Schedule your IOP or weekly therapy sessions as non-negotiable client meetings. Engage a peer coach. Sample two or three meeting formats and commit to those you will consistently attend.
Weeks 7-12: Refresh, do not coast. Update your relapse prevention plan based on your experiences. Schedule the first meaningful family reintegration conversation. Consider adding a digital tool for between-session skill-building if it aligns with your needs. The period when you start feeling stable is precisely when your plan needs to remain robust, not become relaxed.
Family involvement without losing your privacy
Family dynamics are complex. For some, family members at home are the most supportive part of their plan. For others, a parent, spouse, or sibling might be the last person they want calling at 9 p.m. to inquire about a meeting. Both scenarios can exist within the same family. Research on family involvement in substance use treatment indicates that loved ones can be powerful assets when engaged effectively. However, families are often excluded from clinical practice, partly due to legitimate concerns about confidentiality and individual autonomy.
You have the autonomy to define the nature of this involvement. A productive starting point is a brief discussion about roles, rather than focusing on diagnoses. Who will be your Sunday-night check-in person? Who will manage practical logistics, such as a ride home from a late flight or ensuring a quiet house on a difficult anniversary? Who should be on a "do-not-brief" list because the relationship requires healing before it can support recovery discussions? Addressing these points in the second week can prevent well-intentioned but intrusive inquiries that might push individuals away from their own homes.
You can share your schedule without disclosing clinical details. Stating, "I have therapy on Tuesdays and a coach on Thursdays," is sufficient. Your therapist's notes are private.
Digital tools and concierge coordination
Mobile apps and remote check-ins
Between a Tuesday IOP session and a Thursday coach call, you have approximately 160 hours of your own life. This is where digital tools prove invaluable. A recent randomized trial protocol for a self-guided mobile app, which delivers cognitive-behavioral and motivational strategies for individuals addressing addictive disorders, highlights how discreet, remote, on-your-phone support can integrate into a demanding schedule when a therapist's office visit cannot. The same protocol candidly acknowledges limitations: adherence can decline, digital tools are not a substitute for therapist-guided care, and the evidence base is still developing.
Utilize apps as supplementary aids, not as the primary structure of your recovery. This could include a craving log you consistently use, a five-minute grounding exercise before a flight, or a private way to document a challenging moment to discuss in your next therapy session. If an app becomes your sole source of support, it signals a need to incorporate human interaction rather than simply adding more features.
Case management as the connective layer
This is a crucial element often overlooked in discharge planning. You likely have multiple contacts: a prescriber, a therapist, an IOP team, a coach, a sponsor, a spouse, an assistant, and a calendar that constantly shifts. Someone needs to manage these connections. If that responsibility falls entirely on you, the plan is likely to unravel during a week of extensive travel or missed appointments.
SAMHSA's advisory on comprehensive case management directly addresses the importance of this layer. Case management has been shown to help individuals remain engaged in treatment and recovery by coordinating practical aspects such as transportation, housing, medical care, and childcare, thereby creating space for clinical work to progress. For a professional, a case manager or care coordinator is the individual who ensures outpatient appointments are rescheduled when a deposition runs long, confirms communication between your prescriber and therapist, arranges safe transport after a red-eye flight, and protects your privacy by keeping your name off unnecessary systems.
This relationship-based, concierge model of coordination differs significantly from a program-based handoff. It offers a single point of contact, one person who understands the complete picture and adjusts it as your schedule changes. If your current plan lacks this layer, you are effectively acting as your own case manager, a role that can be more demanding than it appears.
When something slips: adjusting the plan without starting over
The immediate response should be contact, not shame. Reach out to your prescriber, therapist, or coach on the same day, prioritizing based on clinical urgency. If you are on medication for opioid or alcohol use disorder, do not discontinue it independently. Continuity of care is most critical in the hours following a slip.
Subsequently, consider briefly escalating your level of support. This might involve:
- Adding two IOP sessions per week for a month
- Temporarily moving into recovery housing
- Increasing coach contact from weekly to daily check-ins
Continuing care research consistently shows that proactive, assertive outreach and sustained engagement lead to better outcomes than passive follow-up. Do not hesitate to ask for additional support; it is a mechanism for success, not a sign of weakness.
Update your relapse prevention plan with the specifics of what occurred: the trigger, the time, the individuals involved, and the narrative you told yourself. This updated document will be one of the most useful tools you create this year.
Frequently Asked Questions
How long should continuing care last after rehab?
Aim for at least a year of active engagement, with the first three months being a critical minimum. NIDA's training principles suggest that roughly three months of continuous treatment often leads to significant improvement, and research consistently shows that longer, actively engaged follow-up yields better outcomes than brief transitions.
Do I have to join a 12-step group to stay sober?
No. While 12-step fellowships are well-supported by evidence, free, and widely available, alternatives like SMART Recovery and LifeRing also exist. Research indicates that matching individuals to the format they prefer is key, as sustained participation is what drives positive outcomes. Sample a few options to find what best fits your schedule and preferences.
Is sober living worth it if I already have a stable home?
Sometimes, yes. If your home environment presents high-risk cues, if a partner is still engaging in substance use, or if travel and isolation pose significant challenges, a three-to-six-month stay in recovery housing can provide crucial support. A long-running study showed that residents experienced measurable improvements in substance use, employment, and psychiatric symptoms over time. It should be viewed as a strategic support, not a demotion.
What should I ask for when I meet with my outpatient team?
Ask three main questions: What is the planned cadence of care for the next 12 weeks? Who will coordinate communication between your prescriber and therapist? What is the plan if cravings intensify or if you experience a slip? If medication for opioid or alcohol use disorder is appropriate but not offered, inquire about the reasons and what might lead to its consideration.
How do I involve my family without giving up my privacy?
Focus on defining roles rather than sharing clinical diagnoses. Communicate your schedule, such as "therapy on Tuesdays, coach on Thursdays," without delving into clinical details. Designate one trusted individual for Sunday-night check-ins and, if necessary, place others on a "do-not-brief" list if those relationships need healing first. Research confirms that families can be valuable assets when engaged appropriately, and it acknowledges that confidentiality concerns are valid and should be openly addressed.
What happens if I slip or relapse during the first year?
Contact your prescriber, therapist, or coach on the same day, prioritizing based on clinical urgency. Do not stop medication independently. Consider increasing your level of support for a month, whether that means additional IOP sessions, temporary recovery housing, or daily coach check-ins. A 2025 review of post-discharge relapse emphasizes that the correct response is to increase support, not decrease it.
References
- Continuing Care Research: What We've Learned and Where We're Going. https://pmc.ncbi.nlm.nih.gov/articles/PMC2670779/
- Aftercare, Relapse Prevention and Continuing Care: Applying Research Findings to Practice. https://www.wicourts.gov/courts/programs/problemsolving/docs/aftercarerelapseprevention.pdf
- National Helpline. https://www.samhsa.gov/find-help/helplines/national-helpline
- Using SAMHSA Funds to Implement Evidence-Based Contingency Management Services. https://library.samhsa.gov/sites/default/files/contingency-management-advisory-pep24-06-001.pdf
- What Did We Learn from Our Study on Sober Living Houses and Where Do We Go from Here?. https://pmc.ncbi.nlm.nih.gov/articles/PMC3057870/
- Peer Recovery Support Services and Recovery Coaching for Substance Use Disorder: A Systematic Review. https://pmc.ncbi.nlm.nih.gov/articles/PMC12811009/
- Evaluating the Effectiveness of Mobile App-Based Self-Guided Psychological Intervention on Addictive Disorders: Study Protocol. https://pmc.ncbi.nlm.nih.gov/articles/PMC10500479/
- Family Involvement in Treatment and Recovery for Substance Use Disorders among Youth. https://pmc.ncbi.nlm.nih.gov/articles/PMC8380649/
- Risk of Relapse Following Discharge from Non-Hospital Residential Treatment Programs for Opioid Use Disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC12035408/
- Comparison of 12-Step Groups to Mutual Help Alternatives for Alcohol Use Disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC5193234/
- Precision in Addiction Care: Does It Make a Difference?. https://pmc.ncbi.nlm.nih.gov/articles/PMC4654192/
- Impact of Continuing Care on Recovery From Substance Use Disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC7813220/
- Chapter 3. Intensive Outpatient Treatment and the Continuum of Care. https://www.ncbi.nlm.nih.gov/books/NBK64088/
- Treatment and Recovery. https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction/treatment-recovery
- Treatment of Substance Use Disorders (NIDA training module). https://webcampus.med.drexel.edu/nida/module_1/content/5_0_Treatment.htm
- Comprehensive Case Management for Substance Use Disorders and Co‑Occurring Disorders. https://library.samhsa.gov/sites/default/files/PEP20-02-02-013.pdf
- Counselor's Treatment Manual: Matrix Intensive Outpatient Treatment for People With Stimulant Use Disorders. https://library.samhsa.gov/sites/default/files/sma13-4152.pdf
A Voice Shaping the Conversation
The topics explored here—change, self-awareness, recovery, and growth—are the same themes Amanda Marino brings to audiences nationwide through speaking engagements and live events.
Known for her appearances on A&E’s Intervention and Digital Addiction, Amanda speaks to organizations, communities, and leadership teams about navigating adversity, embracing vulnerability, and building lives rooted in purpose. Her message resonates far beyond treatment, offering insight that applies to families, professionals, and anyone standing at a crossroads.



Heal on your terms—any time, anywhere.