
How to Have an Intervention: A Compassionate Guide

Key Takeaways
- An intervention is a weeks-long, family-led process of preparation, education, and follow-through — not a televised ambush or a single dramatic evening that decides everything.
- Spend the preparation weeks documenting specific behaviors, learning the six stages from notice through follow-through, and choosing three to six people who can stay calm and on script.
- Compare the Johnson Model, CRAFT, and BSFT honestly — CRAFT is linked to higher treatment entry among initially resistant loved ones and is often the better first move for adult children.4
- A planned family process measurably improves outcomes: treatment involving significant others produced increased effect in reducing substance use above individual therapy or usual care.3
- Open with 'Can we talk?' and hold a four-part structure — connection, specifics, impact, invitation — keeping the tone judgment-free so your adult child can stay in the room.6,5
- Treat 'no' as a stage of change, not a verdict; keep the relationship warm, hold named boundaries, and let small openings count as movement.12
- After yes, stay close through treatment entry and family therapy — continued family involvement is one of the strongest predictors of retention.9,8
- Shift specific financial and reinforcement patterns with a therapist's guidance rather than issuing abrupt cutoffs, since planning costs less than the recurring price of crises.8,11
What an Intervention Actually Is (and Isn't)
If you've spent any time watching reality television, you probably picture an intervention as a tearful living-room ambush — relatives in a semicircle, a stranger with a clipboard, a packed suitcase by the door. That image has done a lot of damage. It's made families feel like they failed when the scene didn't go that way, and it's convinced many adult children that anyone who says "we need to talk" is about to corner them.
Here's the truer picture. An intervention is a planned, family-led process designed to help your adult child consider treatment — and it spans weeks, not a single evening. Family involvement works across the whole continuum of care, from the first nervous conversation through treatment entry and the long stretch of continuing care that follows. The talk itself is one moment inside a much longer arc.1
What an intervention is: preparation, education, a shared message delivered with care, and a real treatment option already lined up before anyone sits down.
What it isn't: a surprise, a punishment, a list of threats, or a one-shot fix. It isn't a moral verdict on your son or daughter, and it isn't a sign that you've waited too long.
If you've already tried talking and it went sideways, you're not failing. You're learning what this family needs next — and that learning is the work.
Before the Conversation: The Weeks That Matter Most
Reading the Signs in Your Adult Child
You probably already know something is wrong. Parents almost always do. The question isn't whether your instinct is right — it's whether you can describe what you're seeing in specific, behavioral terms instead of vague worry.
Watch for patterns, not single bad nights. A son who used to call every Sunday and now goes dark for three weeks. A daughter whose explanations stop tracking — money that disappears, jobs that end suddenly, friendships that quietly fall away. Sleep schedules that have flipped. Weight changes you can see across a holiday visit. New defensiveness around the bathroom door, the medicine cabinet, the car.
Write it down. Dates, what you saw, what was said. Not as evidence to use against your child — as a record for yourself, because shame and gaslighting will make you doubt your own eyes by week three.
And notice the co-occurring signals. Many adult children dealing with substance use are also living with anxiety, depression, trauma, an eating concern, or something undiagnosed underneath. What looks like one problem is often two layered on top of each other. That matters now, because it will shape who you bring in to help and what kind of treatment you start looking into.
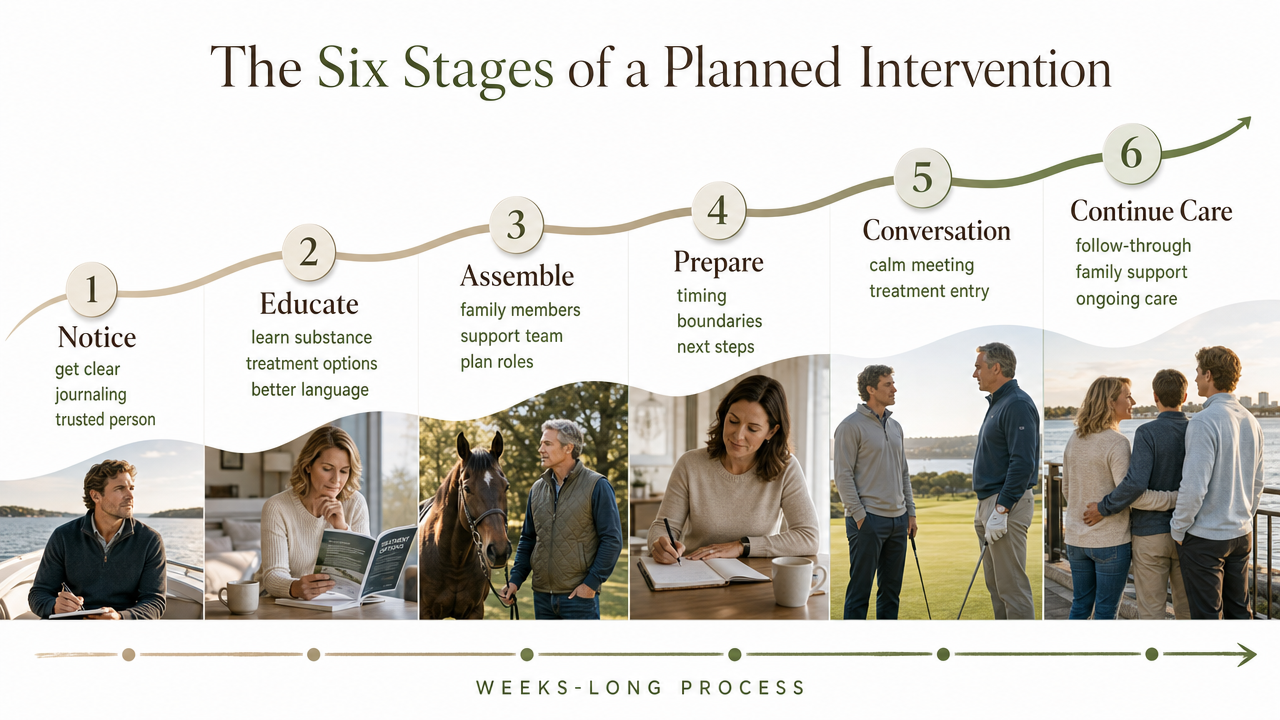
The Six Stages of a Planned Intervention
A real intervention has shape. It moves through stages, and the conversation itself is only one of them. The strongest outcomes come when families treat this as a weeks-long process spanning engagement, treatment entry, and continuing care — not a single dramatic evening.1
Here is the arc most well-planned interventions follow:
- Notice. You name what you're seeing, to yourself and to one other trusted person. This is where the private journaling from the last section becomes useful. You are not building a case. You are getting clear.
- Educate. You and the family members who will be involved learn what you're actually dealing with — the substance or behavior, the typical course, the treatment options that exist, the language to use and the language to drop. This is often where parents first encounter terms like CRAFT or family therapy.
- Assemble. You decide who will be part of the conversation and who won't. You reach out to a facilitator if you're using one. You begin lining up a real treatment option so that "yes" has somewhere to go.
- Rehearse. You practice what each person will say. Out loud. With someone playing your child if possible. This sounds awkward and it is — and it's the single biggest predictor of whether the day itself stays on the rails.
- Convene. The conversation happens. It is calmer than you expect, or harder than you expect, or both in the same hour.
- Follow-through. Whatever your child says, the family keeps moving — into treatment, into family therapy, into a longer plan. This stage is where most outcomes are actually won or lost.
Who Belongs in the Room — and Who Doesn't
Smaller is almost always better. Three to six people, maximum. Each one should have a current relationship with your adult child, a steady emotional baseline, and the discipline to stick to the script you'll build together.
Good candidates: a co-parent or spouse you're aligned with, a sibling your child still talks to, a close family friend or godparent who has been around for years, sometimes an employer or a clergy member if the relationship is real. Adult grandchildren occasionally, with care.
Who doesn't belong in the room: anyone who is currently in active conflict with your child, anyone using heavily themselves, anyone who can't keep their own emotions contained for ninety minutes, and anyone whose presence will read as ambush — the cousin your daughter hasn't seen since high school, the uncle she's afraid of.
If you're working with a trained facilitator, they will push back on your list, and you should let them. The instinct to add one more person "so they hear it from everyone" almost always backfires. The goal is a room your child can stay in — not a courtroom.
Choosing a Model: Surprise Confrontation vs. CRAFT vs. BSFT
Why the Television Version Usually Backfires
The surprise-ambush model — sometimes called the Johnson Model — is what most families picture because it's what cable TV trained them to picture. A facilitator stages a room, the family reads scripted letters, and the loved one is asked to leave for treatment that same day or face named consequences.
It can work. It also has a real failure mode that televised edits don't show you. When your adult child walks into a room and feels cornered by people they trust, the nervous system reads it as a threat. Some leave. Some agree under pressure and then disengage from treatment within days. Some never let their guard down with the family again.
For parents of adult children, the cost of that backfire is heavier than for a teenager still living at home. You don't have the leverage of a curfew or a car key. What you have is the relationship — and you cannot afford to spend all of it in one afternoon.
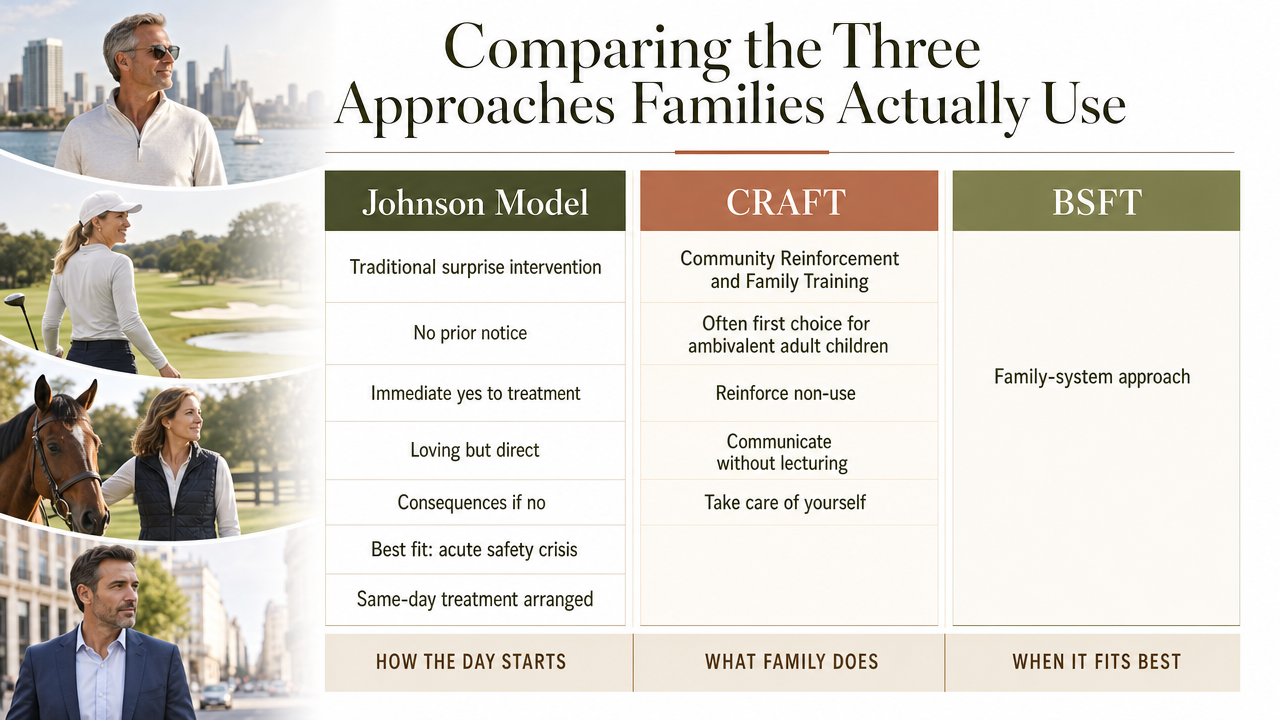
Comparing the Three Approaches Families Actually Use
Three models show up again and again in serious family planning conversations. They aren't interchangeable, and the differences matter for how the day feels and what happens after.
The Johnson Model (traditional surprise intervention).
Family and facilitator gather, your child is invited in without prior notice, and the group asks for an immediate yes to treatment. Tone is loving but direct, with named consequences if the answer is no. Best fit: an acute safety situation where someone is in clear medical danger and a same-day handoff to treatment is already arranged.
CRAFT — Community Reinforcement and Family Training.
This is the model most clinicians now reach for first with adult children who are ambivalent. CRAFT trains you, the parent, in specific skills: reinforcing non-use, communicating without lecturing, taking care of yourself, and creating the conditions in which your child chooses treatment. It is not a single event. There is no ambush. Research links CRAFT to higher treatment entry rates among loved ones who initially resisted help, compared with confrontation-based or detachment-only approaches.
Best fit: your adult child is using, knows you're worried, and has so far said no.4
Brief Strategic Family Therapy (BSFT).
BSFT is a structured family therapy delivered by a trained clinician that targets the patterns inside the family system — who talks to whom, what gets avoided, how conflict is handled. It's part of the broader evidence base for family-involved substance use treatment, which also includes Behavioral Couples Therapy and other family approaches. Studies show BSFT can reduce substance use across both generations in a family and improve family functioning.2,10
Best fit: after the initial conversation, especially when there are co-parents, siblings, or long-running family dynamics that will pull your child back toward use if left unaddressed.
Many families end up combining approaches — CRAFT to get to the conversation, a facilitator to hold the conversation itself, and BSFT or another family therapy in the months after. The chart below lays out the three side by side so you can see which one fits where you are right now. Take a hard look at the column on tone before you decide. If your adult child has already shut down once on you, a surprise confrontation is rarely the right next move.
Why a Planned Family Process Works
Here's the part that surprises most parents: the family isn't just a support system around the treatment. The family is part of the treatment.
A University of Maryland research brief summarizing meta-analytic findings reports that treatment involving significant others produced an increased effect in reducing substance use above and beyond individually-based therapies or usual care. Read that twice. Bringing the people who love your child into the process doesn't just make the family feel better — it measurably improves what happens to your child.3
There are a few reasons this holds up across studies. A planned process gives your adult child time to move from "no, I'm fine" toward "maybe something needs to change" — the slow turn from precontemplation to contemplation that almost never happens in a single dramatic moment. It also changes the environment your child returns to between conversations. The same kitchen, the same Sunday calls, the same patterns — but with different responses from you, informed by what you've learned.
And it shifts the question your child is being asked. Not "will you submit to this room right now?" but "will you let the people who love you stay close while you figure this out?" Those are very different questions. Adult children say yes to the second one far more often than the first.
Insight Beyond Treatment
At Next Level Wellness & Behavioral Health, we believe meaningful change starts with perspective, not just protocols.
That philosophy is directly led by Amanda Marino, whose voice in behavioral health extends beyond clinical settings into leadership, culture, and personal growth.
Through keynote speaking and live events, Amanda explores the deeper themes that show up in recovery, family systems, and life transitions: authenticity, resilience, accountability, and the courage to change. Her work invites audiences to move past labels and into honest conversations that create lasting impact.
The Conversation Itself: Language Parents Can Actually Use
Opening With Three Words: 'Can We Talk?'
You don't need a speech. You need an opener that doesn't trigger the defensive crouch your adult child has been practicing for years.
SAMHSA's family guidance recommends starting with three simple words: "Can we talk?". That's it. No "we need to discuss something serious," no "sit down, this is important," no email subject line that telegraphs an ambush before your son or daughter walks in the door.6
The reason it works is small and quietly powerful. "Can we talk?" is a question, not a verdict. It asks for consent. It puts your adult child in the position of agreeing to a conversation rather than being summoned to one. And it signals — before you've said anything else — that you're approaching this as their parent, not their judge.
Pick a sober moment. Mid-morning on a quiet day is better than after dinner on a Sunday when emotions are already high. In person if possible, by phone if not. And then stop talking and let them answer.
A Short Script Structure That Holds Up Under Stress
Once your child says yes, you have maybe two minutes before instinct takes over and you start lecturing. Hold the structure. A script that survives a tense kitchen has four moves, in order.
- Connection. Start with the relationship, not the problem. "You're my son. I love you. Nothing in this conversation changes that." Say it because it's true, and because they need to hear it before anything else lands.
- Specifics. Name two or three things you've actually seen — not interpretations, not diagnoses. "I noticed you didn't make it to Thanksgiving. I noticed the call last Tuesday where your speech was slurred." Behaviors, dates, what you saw with your own eyes. The journal from your preparation work pays off here.
- Impact. Tell them what watching this has been like for you, briefly. Not to guilt — to be honest. "I've been scared. I haven't slept well in months."
- Invitation. Ask, don't demand. "Will you let me help you look at some options?"
Keep each move short. Two sentences, maybe three. SAMHSA's family materials are clear that the tone should be judgment-free and loving — that's not a soft preference, it's the condition under which your adult child can actually stay in the room with you. The moment your voice tightens into prosecution, the conversation is over even if no one has stood up yet.5
Naming a Real Next Step, Not an Ultimatum
Here is where most family conversations collapse. You've done the connection, the specifics, the impact. Your adult child is still in the chair. And then you say something like, "You need to get help" — and the conversation dissolves into abstraction, because "help" is a word, not a door.
Give them a door. A real one. "I've talked with a counselor who can see you Thursday at 2." "There's an outpatient program twenty minutes from here that has an opening this week." "I'd like you to call this number with me, right now." SAMHSA's National Helpline runs free, confidential, and 24/7 for exactly this moment 7.
The difference between a next step and an ultimatum is the difference between "will you try this with me?" and "or else." Ultimatums put your child's pride on the table alongside their recovery, and pride almost always wins that fight. A concrete invitation, with the logistics already handled, lets them say yes to something small without surrendering anything.
When the Answer Is No (or Not Yet)
Your son shakes his head. Your daughter says she'll think about it and then stops returning calls. The room you spent weeks preparing empties out, and nothing has changed on paper.
Breathe. This is not the end of the story, and it is not a failure of your planning. It is a stage of change with a name. The shift from precontemplation — "I don't have a problem" — to contemplation — "maybe something needs to change" — rarely happens in one sitting. SAMHSA's guidance on this stage emphasizes raising doubt gently, exploring the gap between your child's stated values and their current life, and using empathy rather than pressure to support their own reasons for change.12
That means the work after "no" looks different than the work before it. You keep the door open. You stay in regular, non-loaded contact — a text about the dog, a check-in that isn't about treatment. You hold the boundaries you named without weaponizing them. And you stay in motion yourself: a CRAFT-trained clinician, your own therapist, a family support group.
A "not yet" is information, not a verdict. Many adult children say no the first time and yes the third — sometimes after a smaller crisis, sometimes after watching a parent quietly change. Count what counts: they took the call. They read the brochure. They asked one question. Every one of those is movement.
After 'Yes': Treatment Entry, Family Therapy, and Retention
The yes is a beginning, not a finish line. Most parents exhale, drive their son or daughter to the assessment, and assume the professionals take it from here. That handoff is where a lot of families quietly disengage — and where outcomes start to slip.
Stay close. Family involvement is one of the strongest predictors of whether someone actually stays in treatment long enough for it to work. The University of Washington's retention research is blunt about it: most patients engage in treatment because of positive family involvement, and continued engagement keeps them there. Your job didn't end at the front door of the program.9
Ask the clinical team about family therapy from week one. SAMHSA's TIP 39 frames family counseling as a core part of substance use treatment, not an add-on — focused on communication, boundaries, and shared problem-solving across the system your child is returning to. If the program doesn't offer it, find a family therapist who does, in parallel.8
And protect the long view. Treatment entry is one stage in a continuum that includes early recovery, relapse risk, and continuing care. Show up for the family sessions. Keep the Sunday calls. Celebrate the small wins out loud — a full week, a kept appointment, a hard conversation that didn't end in a slammed door.1
Boundaries, Financial Entanglement, and the Limits of Parental Authority
Here's the part nobody warns you about: your adult child is an adult. You can't sign them into treatment. You can't take their phone. You can't ground them. Whatever leverage you had at sixteen is gone, and pretending otherwise will cost you the conversation.
What you do still control is your own behavior — which is exactly where CRAFT-style work focuses parents. The rent check. The car insurance you've been quietly paying. The credit card on the account. The guest room that's been available since the layoff. None of these are punishments. They are choices you've been making, and you get to make different ones.4
Boundaries land differently when they are specific, consistent, and named in advance. "I love you, and I won't transfer money for groceries anymore — I'll bring groceries instead" is a boundary. "I'm done with you" is a threat. One keeps the relationship intact while changing the reinforcement pattern around use. The other ends the conversation.
SAMHSA's TIP 39 frames this as part of healthy family functioning — clearer roles, cleaner communication, less of the silent enabling that long-term family stress tends to produce. Talk it through with a family therapist before you announce anything. Pulled too fast, financial boundaries can trigger a crisis without a treatment door open. Held firm with a plan, they create the conditions where yes becomes the easier answer.8
What Planning Well Costs You — and What Not Planning Costs More
Let's be honest about money for a minute, because nobody else will be. Planning a real intervention costs something. A trained facilitator, a few sessions with a family therapist, an outpatient assessment, maybe travel — these are real line items, and you'll see them on a credit card statement.
Now look at the other column. The ER visits you've already paid for. The bailed-out lease. The wrecked car. The lost job that landed back on your kitchen. Crises are expensive, and they keep billing you. A systematic review of family-based substance use interventions found the majority were cost-beneficial compared to doing nothing.11
Planning well is the cheaper path. It just asks you to pay on purpose.
For support that meets you right where you are—anytime, anywhere—connect with us today.
Frequently Asked Questions
Do we need a professional interventionist, or can our family do this alone?
Some families do this well on their own, especially with CRAFT-style coaching for one or both parents. Bring in a trained facilitator when stakes are high — repeated attempts, safety concerns, co-occurring mental health issues, or a family that can't stay aligned in the same room. A facilitator buys you steadiness when emotions surge.4
What's the difference between CRAFT and a traditional intervention?
A traditional intervention is a single planned conversation, often with the element of surprise, asking for an immediate yes to treatment. CRAFT is a longer coaching process that trains you in communication and reinforcement skills so your adult child moves toward treatment on their own terms. CRAFT is linked to higher treatment entry among initially resistant loved ones.4
What do we do if our adult child refuses treatment after the conversation?
Treat "no" as a stage, not a verdict. SAMHSA's motivational guidance describes the move from precontemplation to contemplation as gradual — built through gentle doubt, empathy, and values-based conversation rather than pressure. Keep the relationship warm, hold the boundaries you named, stay in your own coaching or therapy, and let small openings count.12
Should we cut off financial support as part of the intervention?
Not abruptly, and not as a threat. Sudden financial cutoffs without a treatment door open can trigger a crisis. Work with a family therapist to shift specific reinforcement patterns — groceries instead of cash, paid rent instead of transferred funds — in a way that's named in advance and consistent. TIP 39 frames this as healthy family functioning.8
Who should — and shouldn't — be in the room during the conversation?
Three to six people, each with a current relationship with your adult child and the discipline to stay on script. A co-parent, a trusted sibling, a long-time family friend. Leave out anyone in active conflict, anyone using heavily themselves, and anyone whose presence will read as ambush. Smaller rooms hold up better under stress.
How long does an intervention actually take from start to finish?
Plan for weeks, not an evening. Notice, educate, assemble, rehearse, convene, and follow through — most families spend four to eight weeks before the actual conversation, and then months of family therapy and continuing care after. Family involvement works across the full continuum of care, not as a one-time event.1
References
- Family Involvement in Treatment and Recovery for Substance Use Disorders: A Narrative Review and Conceptual Framework. https://pmc.ncbi.nlm.nih.gov/articles/PMC8380649/
- Evidence-based practices for substance use disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC3678283/
- Engaging Family and Others in Recovery | Research Corner. https://iris.ssw.umaryland.edu/rc-family-recovery
- Community Reinforcement and Family Training (CRAFT): Community Reinforcement Approach (CRA) and CRAFT. https://www.ncbi.nlm.nih.gov/books/NBK64952/
- Helping a Loved One Dealing with Mental and/or Substance Use Disorders. https://www.samhsa.gov/sites/default/files/samhsa_families_family_support_guide_final508.pdf
- Helping Families Cope with Mental Health and Substance Use. https://www.samhsa.gov/mental-health/children-and-families/coping-resources
- National Helpline for Mental Health, Drug, Alcohol Issues - SAMHSA. https://www.samhsa.gov/find-help/helplines/national-helpline
- Chapter 3—Family Counseling Approaches (TIP 39: Substance Use Disorder Treatment and Family Therapy). https://www.ncbi.nlm.nih.gov/books/NBK571088/
- Retention Toolkit: Family Involvement. https://adai.uw.edu/retentiontoolkit/family.htm
- The effects of Brief Strategic Family Therapy (BSFT) on parent substance use and adolescent substance use. https://pmc.ncbi.nlm.nih.gov/articles/PMC4370509/
- Family-based Interventions to Prevent Substance Use Among Youth: Economic Evaluations. https://pmc.ncbi.nlm.nih.gov/articles/PMC12185227/
- Chapter 4—From Precontemplation to Contemplation (TIP 35: Enhancing Motivation for Change in SUD Treatment). https://www.ncbi.nlm.nih.gov/books/NBK571072/
A Voice Shaping the Conversation
The topics explored here—change, self-awareness, recovery, and growth—are the same themes Amanda Marino brings to audiences nationwide through speaking engagements and live events.
Known for her appearances on A&E’s Intervention and Digital Addiction, Amanda speaks to organizations, communities, and leadership teams about navigating adversity, embracing vulnerability, and building lives rooted in purpose. Her message resonates far beyond treatment, offering insight that applies to families, professionals, and anyone standing at a crossroads.



Heal on your terms—any time, anywhere.