
Understanding Positive Life Transitions in Recovery

Key Takeaways
- A positive transition is structural, not emotional — SAMHSA's four dimensions of health, home, purpose, and community are the load-bearing pieces to inventory and reinforce 1.
- The weeks after discharge are the most fragile seam, when tolerance has dropped and aftercare is still assembling, so appointments, medications, and a named contact belong on paper before day one 11.
- Support roles are not interchangeable: recovery companions, case managers, peer mentors, sponsors, and informed family each do different work, and scheduled clinical contact improves treatment engagement 4, 7.
- Focus next on building recovery capital through consistent mutual-help attendance, phased returns to work or school, planned handling of unstructured time, and pre-scripted plans for weddings and holidays 3, 12.
What Actually Changes When You Walk Out the Door
The door closes behind you. The parking lot is quiet. Someone has your bag, or you do, and the next hour is unstructured for the first time in weeks. That moment — not the discharge paperwork, not the last group — is where the transition actually starts.
Here is what shifts. The scaffolding disappears. No one hands you a schedule at breakfast. No one notices if you skip a meal or stay up too late. The people who knew your name and your story are back to their own days, and you are back to yours, which does not yet have a shape.
This is not failure. This is the design of the moment. Recovery, as SAMHSA defines it, is a long process of change through which you improve your health, live a self-directed life, and work toward your full potential — not a finish line you cross at discharge 1. What you are stepping into is the self-directed part, and it is supposed to feel unfamiliar.
The rest of this piece is a map of that unfamiliar ground: what the research says helps in the first weeks, who the people around you actually are, and how to build a week you can stand inside.
The First Weeks: The Window Nobody Warned You About
Why the Handoff From Treatment to Home Is the Riskiest Seam
The first few weeks after discharge are not just emotionally loaded. They are structurally fragile. Inside treatment, someone else held the schedule, the meds, the meals, the check-ins. Outside, all of that is on you, and the systems that are supposed to catch you — outpatient therapist, prescriber, primary care, a group you can walk into — are often not yet threaded together on day one.
That seam is where things slip. A review of transitions of care for substance use disorders puts it plainly: safe handoffs require timely communication between providers, coordination of services, and active linkage to ongoing support, not a discharge summary handed to you at the door 6. When any of those threads goes missing — the referral that never got sent, the intake appointment three weeks out, the prescription that lapsed — the gap fills with old habits and old people.
You do not have to fix the whole system. You do have to notice, in the first week, whether the appointments actually exist on a calendar, whether someone besides you knows about them, and whether there is a name and number to call when something wobbles at 8 p.m. on a Sunday.
An Honest Word About the Early Mortality Window
What that risk translates to, practically: do not walk into the first week without a plan for medications, without a phone number you will actually call at 2 a.m., and without at least one person who knows where you are sleeping. If opioids were part of your history, the overdose-prevention piece of your aftercare is not optional. Ask about it before you leave.
What a Real Aftercare Plan Looks Like on Paper
An aftercare plan is not a document your treatment team hands you. It is a small, boring, specific list you can hold in one hand and check against reality. If you cannot answer these questions from memory, the plan is not built yet.
- Who is your prescriber, and when is the next appointment? Not "soon." A date on a calendar, within two weeks of discharge, with the medication list confirmed.
- Who is your therapist or outpatient program, and what is the weekly cadence? First session inside seven to ten days is the target.
- What are your two community anchors? A meeting, a group, a peer contact — something you attend on a repeating day, not "when you feel like it."
- Who is the one person who has your schedule? A recovery companion, a case manager, a family member who has done their own work. One human who notices when you go quiet.
- What is the plan for the first bad night? Not the concept of a plan — the actual number to call and the actual place to go.
Recovery Management Checkups research shows that people who get scheduled, ongoing clinical contact spend more days engaged in treatment and fewer days in heavy use than people left to check in on their own 4. Build the calendar. Then hand a copy to someone else.
The People Around You Have Different Jobs
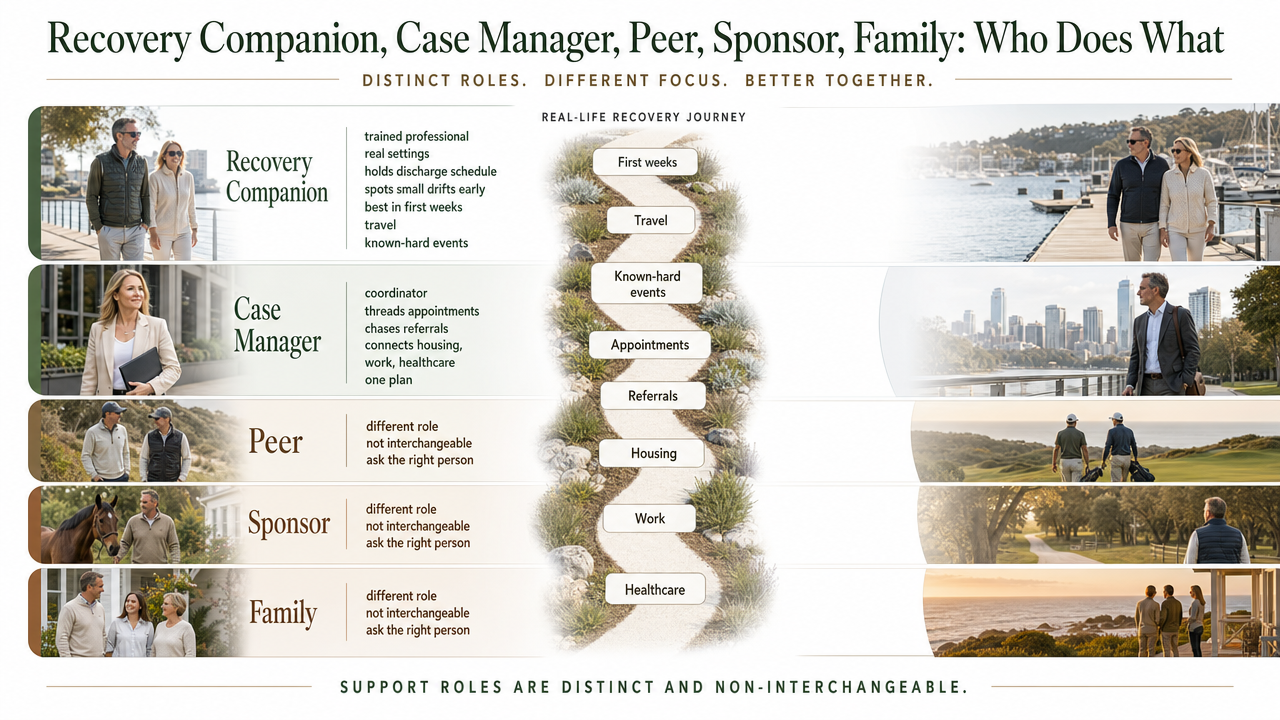
Recovery Companion, Case Manager, Peer, Sponsor, Family: Who Does What
"Support system" is a phrase that hides more than it reveals. The people around you are not interchangeable. They have different jobs, different training, and different hours, and if you treat them as one blurry group, you will end up asking the wrong person for the wrong thing at the wrong time.
Here is how to think about the roles.
- Recovery companion. A trained professional who is with you in real settings — your kitchen, the airport, the first dinner out. They hold the schedule you built at discharge and notice the small drifts before they become big ones. Best used in the first weeks, during travel, or around known-hard events.
- Case manager. The coordinator. Threads the appointments together, chases the referral that never got sent, connects housing, work, and healthcare into something that behaves like one plan. A review of case management for substance use disorders links this role to improved linkage to services, reduced use, and better social functioning 7.
- Peer mentor or recovery coach. Someone with lived experience walking a few steps ahead of you. A systematic review of peer support found it associated with reduced substance use, improved retention in treatment, and enhanced quality of life 8. Different from a companion — less about coverage, more about "I have been where you are."
- Sponsor. A relationship inside a mutual-help fellowship. Not a clinician, not paid, not on call in a professional sense — but often the person who takes the 11 p.m. phone call.
- Family. The people who share your history and, ideally, are doing their own work alongside yours. Family involvement is linked to higher treatment retention and lower relapse rates when the involvement is informed and supported 13.
Scheduled clinical contact — the Recovery Management Checkup model — sits above all of this, and research shows people receiving these checkups had more treatment days and fewer heavy-use days than those in standard care 4. Pick roles by function, not by whoever is closest.
Bringing Family Back In Without Rebuilding the Old House
Family is where recovery gets tender. These are the people who watched the hardest years, and coming home means walking back into rooms that hold old scripts — the arguments that had a shape, the dinners that ended the same way, the roles everyone learned to play.
The research is careful and worth hearing. Family involvement, when it is informed and supported, is linked to higher treatment retention, lower relapse rates, and improved family functioning 13. The word doing the work in that sentence is informed. Family members who have done their own reading, their own therapy, their own Al-Anon or family group meetings show up differently than family members who are running on love and fear alone.
A few things that tend to help in the first months at home:
- Name the new house rules together, out loud, before you need them. Not as ultimatums — as agreements. Who knows about appointments. What happens on a hard night. What is off-limits in conversation for now.
- Ask the family members most invested in your recovery to have their own support — a therapist, a group, a coach. Their calm is part of your environment.
- Accept that some old dynamics will try to reassemble themselves. Noticing them is enough at first. You do not have to solve the family in month one.
You are not rebuilding the old house. You are moving into a different one with some of the same people. That distinction is the whole point.
Insight Beyond Treatment
At Next Level Wellness & Behavioral Health, we believe meaningful change starts with perspective, not just protocols.
That philosophy is directly led by Amanda Marino, whose voice in behavioral health extends beyond clinical settings into leadership, culture, and personal growth.
Through keynote speaking and live events, Amanda explores the deeper themes that show up in recovery, family systems, and life transitions: authenticity, resilience, accountability, and the courage to change. Her work invites audiences to move past labels and into honest conversations that create lasting impact.
Rebuilding Weekly Rhythm: Work, School, and the Question of Purpose
Returning to Work Without Making It a Test
Work is one of the load-bearing pieces. Research on employment and recovery links stable work to better recovery outcomes, reduced substance use, and improved psychosocial functioning — not because a paycheck is magic, but because a workweek gives you structure, purpose, and financial ground under your feet 12.
That said, the first month back is not a proving ground. You are not there to make up for lost time or perform how well you are doing. You are there to build a repeatable week.
A few things to hold onto:
- Start with fewer hours than you think you can handle. A part-time reentry, or a phased return, lets you protect sleep, appointments, and evening recovery time. You can always add hours in month three.
- Decide in advance who at work needs to know what. The answer is often "almost no one." A trusted manager or HR contact is usually enough. Disclosure is a choice, not a duty.
- Protect the therapy hour on the calendar. If it moves for a meeting, it moves once, not twice.
If work was tangled up with your hardest years — the after-hours culture, the travel, the specific bar around the corner — the honest question is not whether to go back, but whether to go back to the same shape of it.
If You're Going Back to School
School has its own weather. The unstructured afternoons, the social scripts built around drinking, the pressure of a syllabus that assumes you have been in one continuous life for four years — all of it can catch you off guard.
Collegiate recovery programs exist for exactly this reason. Research on campus-based recovery communities describes housing, counseling, peer support, and sober social activities as a package designed to hold students inside recovery while they pursue a degree, with a social environment supportive of recovery treated as essential to sustaining a substance-free lifestyle 2.
If your campus has one, walk in during the first week. If it does not, build the equivalent yourself: one meeting on or near campus, one sober friendship intentionally cultivated in the first month, a housing situation that is not the loudest dorm on the loudest floor, and a therapist you keep seeing even when midterms hit. The degree is the goal. The scaffolding is what gets you to it.
Tuesday at 3 P.M.: Handling Unstructured Time
Nobody warns you about Tuesday at 3 p.m. The mornings have a shape — coffee, appointment, gym, a task list. The evenings have meetings, dinner, a call with your sponsor. It is the middle of the afternoon on an ordinary weekday that tends to catch people flat.
Unstructured time is not the enemy. Unplanned unstructured time is. There is a difference between an afternoon you chose to leave open and an afternoon that opened up on you.
Try this. Once a week, on Sunday night, look at the coming seven days and find the soft spots — the afternoons, the Saturday morning, the long stretch after work on Thursday. Put something in each one. Not something huge. A walk. A book at a specific café. A phone call to a friend you keep meaning to catch up with. A volunteer shift. A cooking project.
Purpose, in the SAMHSA sense, is not one big calling 1. It is a week that has enough small purposes stitched into it that no single hour has to carry the whole thing.
Community You Can Actually Use
Mutual-Help Groups and What the Research Says About Them
You have probably been told to "find a meeting" more times than you can count. It is worth knowing why the advice keeps getting repeated: it is one of the few community-based supports with a real evidence base behind it.
A systematic review of mutual-help groups for people with drug use disorders found that attendees experienced fewer relapses and higher rates of sustained remission than those in some rehabilitation settings 3. That is not a small finding. It is a room full of strangers, most weeks free, in most neighborhoods, associated with the outcome you are actually trying to protect.
The tradition matters less than the fit. Twelve-step rooms — AA, NA, CA — are the most widespread, but SMART Recovery, Refuge Recovery, LifeRing, and Dharma-based groups all exist, and one of them is probably meeting near you this week. Try three before you decide none of them are for you. The first meeting is almost always the worst one.
One practical note: pick a home group and go on the same day each week for a month before you judge the format. Consistency is where the benefit lives.
Digital and Discreet Options for a Private Life
Not every recovery has to happen in a church basement. If your work, your name, or your circumstances make a public room complicated, you have other doors.
Research on digital recovery support services — moderated online communities, recovery-focused apps, telehealth peer coaching, private video meetings — describes them as extending the reach of recovery support and offering greater accessibility and anonymity than some traditional services 9. For someone protecting a professional identity, a household, or simply their privacy, that matters.
A workable stack often looks like this: one live meeting a week (in person or on a private video call), one app or online community you check most days, and one human — a peer coach or recovery companion — who knows the whole picture. Digital tools are good bridges. They are not meant to carry the weight alone.
The First Wedding, the First Holiday, the First No
Somewhere in the first year, an event you cannot skip will land on the calendar. A cousin's wedding. Thanksgiving at the house where everything used to happen. A work dinner where the wine list is the whole point. The question is not whether these arrive. The question is what you do the week before.
A workable approach has three moving parts.
- Decide who goes with you or who is on call. A recovery companion, a peer, a family member who has done their own work — one person who knows the plan and can leave with you if leaving is the right call.
- Script the sentence. "I'm not drinking tonight" is complete. You do not owe anyone the longer version. Practice it out loud once so it sounds like yours.
- Plan the exit. Your own car, a ride you already booked, a room booked nearby — a way out that does not require a committee vote at 10 p.m.
The first no is the hardest one. The second is easier. By the fifth, you will have a version of yourself that goes to weddings and comes home the same person who left.
A Twelve-Month View You Can Hold in Your Head
Zoom out. A year is not one long stretch — it is four seasons of different work.
- Months 1–3. Stabilize.
- Keep every appointment. Lean on the recovery companion, the case manager, the meeting you picked. Say no to more than you say yes to.
- Months 4–6. Deepen.
- Sponsor or peer relationship gets real. Work or school settles into a rhythm. Recovery capital starts to compound — the second job of building your life, alongside the first job of protecting it 5.
- Months 7–9. Widen.
- New friendships. A hobby that is yours, not borrowed. Family conversations that go somewhere.
- Months 10–12. Consolidate.
- A recovery-oriented view treats this as continuity, not a finish line 10. Keep the checkups. Keep the community. You are not done — you are resourced.
If you want a partner in this — a companion who shows up in real settings, a case manager who threads the plan — that is what Next Level does. Quietly, and on your timeline.
Frequently Asked Questions
What makes a life transition after treatment 'positive'?
A positive transition is not a mood. It is a structure. SAMHSA frames recovery around four dimensions — health, home, purpose, and community — and the more of those you have real weight under, the better your odds of moving forward well 1. You can feel wobbly and still be doing this well, as long as the load-bearing pieces are in place.
How long does the higher-risk period last after leaving residential treatment?
Research on mortality after residential discharge points to elevated risk in the weeks following the transition, when tolerance has dropped and aftercare is still assembling 11. The practical answer: treat the first month as the most fragile seam. Keep prescriber and therapy appointments on the calendar, and make sure one person besides you knows your plan.
What's the difference between a recovery companion, a case manager, a peer mentor, and a sponsor?
A recovery companion is a trained professional who is with you in real settings — home, travel, hard events. A case manager threads appointments, housing, work, and healthcare into one plan and has been linked to better linkage and social functioning 7. A peer mentor walks a few steps ahead with lived experience 8. A sponsor is an unpaid relationship inside a mutual-help fellowship.
When should I return to work or school after treatment?
Sooner than you fear, slower than you think. Stable employment is linked to better recovery outcomes and improved psychosocial functioning, largely because a workweek gives you structure 12. Start part-time or phased. Protect sleep and your therapy hour. If you are going back to campus, look for a collegiate recovery community in the first week 2.
How do I handle the first wedding, holiday, or family event without slipping?
Three moving parts. Decide who goes with you or is on call — a recovery companion, peer, or informed family member. Family involvement is linked to lower relapse rates when it is informed and supported 13. Script the sentence: "I'm not drinking tonight" is complete. And plan your exit before you arrive — your own ride, a room nearby.
Are there discreet recovery support options if I value privacy?
Yes. Digital recovery support services — moderated online communities, recovery apps, private video meetings, telehealth peer coaching — extend the reach of support and offer greater accessibility and anonymity than some traditional settings 9. Paired with a private in-person contact like a companion or case manager, they let you protect a professional identity while still being resourced.
References
- Recovery and Support. https://www.samhsa.gov/substance-use/recovery
- Collegiate Recovery Communities Programs: What do we know?. https://pmc.ncbi.nlm.nih.gov/articles/PMC3952555/
- Effectiveness of Mutual Help Groups for Illicit Drug Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC12360454/
- Recovery Management Checkups for Individuals with Chronic Substance Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC4509252/
- Recovery Capital as Prospective Predictor of Sustained Recovery. https://pmc.ncbi.nlm.nih.gov/articles/PMC3774224/
- Transitions of Care for Patients With Substance Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC4380913/
- Case Management for Patients with Substance Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC5102851/
- Peer Support in Recovery from Substance Use Disorders: A Systematic Review. https://pubmed.ncbi.nlm.nih.gov/28340990/
- Digital Recovery Support Services: Characterizing and Evaluating Online Recovery Communities. https://pubmed.ncbi.nlm.nih.gov/31514089/
- Recovery-Oriented Systems of Care: A Review of the Evidence. https://pubmed.ncbi.nlm.nih.gov/29775466/
- Mortality After Residential Addiction Treatment: Risks During Transition. https://pubmed.ncbi.nlm.nih.gov/26892871/
- Employment as a Component of Recovery from Substance Use Disorders. https://pubmed.ncbi.nlm.nih.gov/30629980/
- Family Involvement in Recovery from Substance Use Disorders. https://pubmed.ncbi.nlm.nih.gov/25043212/
A Voice Shaping the Conversation
The topics explored here—change, self-awareness, recovery, and growth—are the same themes Amanda Marino brings to audiences nationwide through speaking engagements and live events.
Known for her appearances on A&E’s Intervention and Digital Addiction, Amanda speaks to organizations, communities, and leadership teams about navigating adversity, embracing vulnerability, and building lives rooted in purpose. Her message resonates far beyond treatment, offering insight that applies to families, professionals, and anyone standing at a crossroads.



Heal on your terms—any time, anywhere.