
Supporting Employees: Workplace Services in Boca Raton

Key Takeaways
- Boca Raton employers face real access constraints — national clinician shortages and thin regional pipelines mean the two-week gap between decision and first appointment is where senior staff quietly disengage 3, 17.
- Executives and professionals break differently, with isolation and effort-reward imbalance driving a distinct exhaustion signature that standard EAPs rarely reach because senior leaders avoid shared portals 22, 8.
- Durable programs run three layers at once — organizational design, supervisor behavior, and a discreet individual pathway — since participatory interventions hold for 12 months while brief workshops fade by three 9, 18.
- Before signing a concierge partner, compare fees, clinician qualifications, timelines, evaluation methods, confidentiality protections, network coordination, and clinical handoffs — not whether the vendor replaces your existing benefits stack 16.
The Utilization Problem Hiding Inside Your Benefits Stack
You already know your benefits package looks good on paper. Medical coverage, an EAP number tucked into onboarding materials, maybe a meditation app subscription that leadership approved last spring. On the surface, your workforce has what it needs. So why does the phone in HR keep ringing about the same problems — a director who quietly disappeared for two weeks, a VP whose performance has slipped in ways nobody wants to name out loud, a mid-level manager whose team keeps turning over?
Here is the gap most employers miss. Availability is not the same as use. In March 2024, 72% of private industry workers had access to medical care benefits and 79% had access to paid sick leave 4. Coverage is broad. The problem is that the people who need behavioral health support the most — especially senior staff — often will not touch a standard EAP because they fear exposure, career consequences, or a paper trail that runs through their own HR department.
Meanwhile, the workforce reality is stark. Roughly two-thirds of adults with a substance use disorder are employed 2. That means your best salesperson, your CFO, your operations lead — the people carrying the most weight — are the same population statistically most likely to be quietly managing something. The workplace is where recovery either takes hold or unravels.
You are not failing your team by having gaps here. Most professional employers do. What you are looking at is a design problem: the traditional benefits stack was built for volume, not for the discretion and clinical depth a professional workforce actually uses. The rest of this piece is about what closes that gap without dismantling what you already have.
Why Executive and Professional Workforces Break Differently
The Exhaustion Signature at the Top of the Org Chart
Here is something you probably already sense but rarely see named out loud: the people at the top of your org chart are not experiencing the same kind of tired as everyone else. When a systematic review looked specifically at leaders and managers, it concluded that executives and managers show high levels of emotional exhaustion, with organizational culture, role conflict, and workload driving much of the pattern 22. That is a distinct clinical signature — not garden-variety stress, not weekend-can-fix-it fatigue.
You have likely watched it play out. The senior leader who used to run point on the hardest client meetings now delegates them and calls it maturity. The founder who once made decisions in an hour now sits with them for a week. The VP who is technically at their desk but functionally somewhere else. Burnout in this population is strongly linked to high job demands, low control, and insufficient rewards — a combination that describes almost every C-suite role in a competitive market 20.
What makes this population break differently is not just workload. It is the isolation that comes with rank. A director cannot vent to their direct reports. A CFO will not raise a hand in the same all-hands meeting where their team sits. A founder feels like the only person who cannot afford to look uncertain. So the exhaustion compounds in private, and by the time it surfaces, it usually shows up as a performance issue, a health scare, or a resignation letter.
You are not imagining the pattern. The research names it. And once you see it as a distinct clinical signature rather than a character flaw, the response changes — from managing performance to protecting the person who is carrying the weight.
The Psychosocial Machinery Behind the Strain
If exhaustion is the signature, the psychosocial machinery underneath it is the reason the signature keeps repeating across your team. A meta-analysis of stress-related mental disorders found that effort-reward imbalance, low organizational justice, and high job demands were associated with a 60% to 90% increased risk of stress-related mental disorders 8. Read that again slowly. That is not a small effect. That is a near-doubling of risk driven by conditions your organization designs on purpose — comp structures, promotion timelines, decision authority, workload distribution.
The mechanics are unglamorous. Effort-reward imbalance means someone is pouring in far more than they are getting back, and the imbalance persists long enough to become chronic. Low organizational justice means people watch decisions get made in ways that feel arbitrary or political. High job demands means the calendar has more on it than any human can carry. For a senior professional, all three often stack at once, especially during growth stretches, restructuras, or when a team is running lean by design.
What matters for your workplace services strategy is that these are levers you can actually move. A therapist cannot fix a broken comp philosophy. A meditation app cannot reduce a workload. A one-hour resilience webinar cannot repair a manager who never learned to give credit. The strain lives in the design of the work, which is why the more durable interventions target the system alongside the individual.
The good news — and this is the part that gets lost — is that once you see the machinery, you can start adjusting it in small, honest ways. That is where a real program starts.
Boca Raton's Access Reality: Clinician Shortages and Referral Gaps
Here is the part of the picture that changes what your program has to do. Nationally, 122 million people live in a mental health Health Professional Shortage Area 3. That is not a rural problem or someone else's problem — it is the water your workforce is swimming in, including here in South Florida. When your CFO decides on a Tuesday night that she is ready to talk to someone, the wait for a qualified clinician who takes her insurance and can hold a confidential appointment during working hours is often measured in weeks, not days.
Palm Beach County has been working on this from the system side. The county's Crisis Now implementation report explicitly names workforce development as strategically important for behavioral health system success in the region 17. That is a polite way of saying the pipeline is thin, referral coordination is uneven, and the handoff between a crisis contact and sustained care is where people fall through. If you have ever tried to help an employee find a psychiatrist within a reasonable drive of the office, you already know this.
A concierge layer earns its keep in exactly that gap. It is not a replacement for the clinicians in your network or the EAP you already fund. It is the person who picks up the phone Tuesday night, knows which providers actually have openings this week, and coordinates the referral in a way that protects the employee's privacy and their calendar. In a market with real access constraints, that coordination is not a luxury. It is what turns a benefit on paper into help that actually arrives on time.
Insight Beyond Treatment
At Next Level Wellness & Behavioral Health, we believe meaningful change starts with perspective, not just protocols.
That philosophy is directly led by Amanda Marino, whose voice in behavioral health extends beyond clinical settings into leadership, culture, and personal growth.
Through keynote speaking and live events, Amanda explores the deeper themes that show up in recovery, family systems, and life transitions: authenticity, resilience, accountability, and the courage to change. Her work invites audiences to move past labels and into honest conversations that create lasting impact.
What a Program That Actually Moves the Needle Looks Like
One-Off Workshops vs. Sustained Organizational Work
You have probably sat through the ninety-minute resilience webinar. Maybe you paid for it. The room nods, a few people say it was useful, and six months later you cannot point to a single thing that changed. That is not a failure of your team's attention. It is a design problem baked into the format.
Here is the finding that should reshape how you spend your program dollars. A 2025 systematic review of workplace mental health programs found that brief workshops had no sustained effects beyond three months, while participatory organizational interventions reduced burnout for at least 12 months 9. Read that as a straight comparison. The short training that fits neatly into a lunch hour buys you a quarter of measurable effect, and then the curve flattens. The intervention that actually involves employees in reshaping how work gets done — workload distribution, decision authority, recognition patterns — holds for a full year.
Participatory means the people doing the work help redesign it. A team names the friction points. Leadership actually adjusts something in response. The change gets measured, then adjusted again. It is slower than a webinar. It is also the only format the evidence supports as durable.
None of this means you should cancel the training calendar. Manager education still matters, especially around recognizing distress and having accommodation conversations. What it means is that if a workshop is the whole program, you have bought a compliance artifact, not an outcome. The training is the entry point. The organizational work is what actually shifts the numbers.
Give yourself credit for what you have already funded, and give yourself permission to stop expecting a single event to do a year's worth of work. That reframe alone changes how the next budget cycle gets built.
The Three-Layer Architecture: Organization, Supervisor, Individual
The programs that hold up over time share a structure. Three layers, each doing work the other two cannot do alone. When one layer is missing, the whole thing wobbles — which is what happens when an employer stacks an EAP on top of an unchanged workload and calls it a mental health strategy. NIOSH puts this plainly, recommending that workplace programs address environmental determinants of health rather than focusing only or primarily on individual-level interventions 18.
The organizational layer is where the machinery lives. This is policy, workload calibration, decision authority, comp philosophy, and the honest audit of whether your team is running lean by design or by neglect. It is also where you review the psychosocial exposures that quietly drive risk — the effort-reward imbalances, the calendars that pretend a person can be in three places at once. Nobody loves this layer because the fixes are unglamorous and the wins are slow. It is also the layer with the largest effect size on long-term outcomes.
The supervisor layer is where policy becomes behavior. Your managers are the people who notice a change in a team member first, and they are the people who either open a supportive conversation or manage past it. This layer needs real training on recognizing distress, holding an accommodation conversation without turning it into a legal event, and knowing where to hand off. Under the EEOC framework, employees may be entitled to accommodations such as altered work schedules or permission to work from home when needed due to a mental health condition 1. A supervisor who understands that is a supervisor who does not accidentally push a valuable senior contributor toward the exit.
The individual layer is the discreet clinical pathway — coaching, counseling, recovery support, care coordination. This is where a concierge model earns its keep, because for professional and executive populations, the individual layer only works if it is genuinely private and genuinely fast. A CFO will not walk into a group intake. A founder will not use the same portal as their operations team. What they will use is a single point of contact who verifies clinicians, matches level of care, and protects the calendar.
Build all three. Skip any one, and the other two carry weight they were never designed to carry.
A 3-, 6-, and 12-Month Cadence for Measurable Change
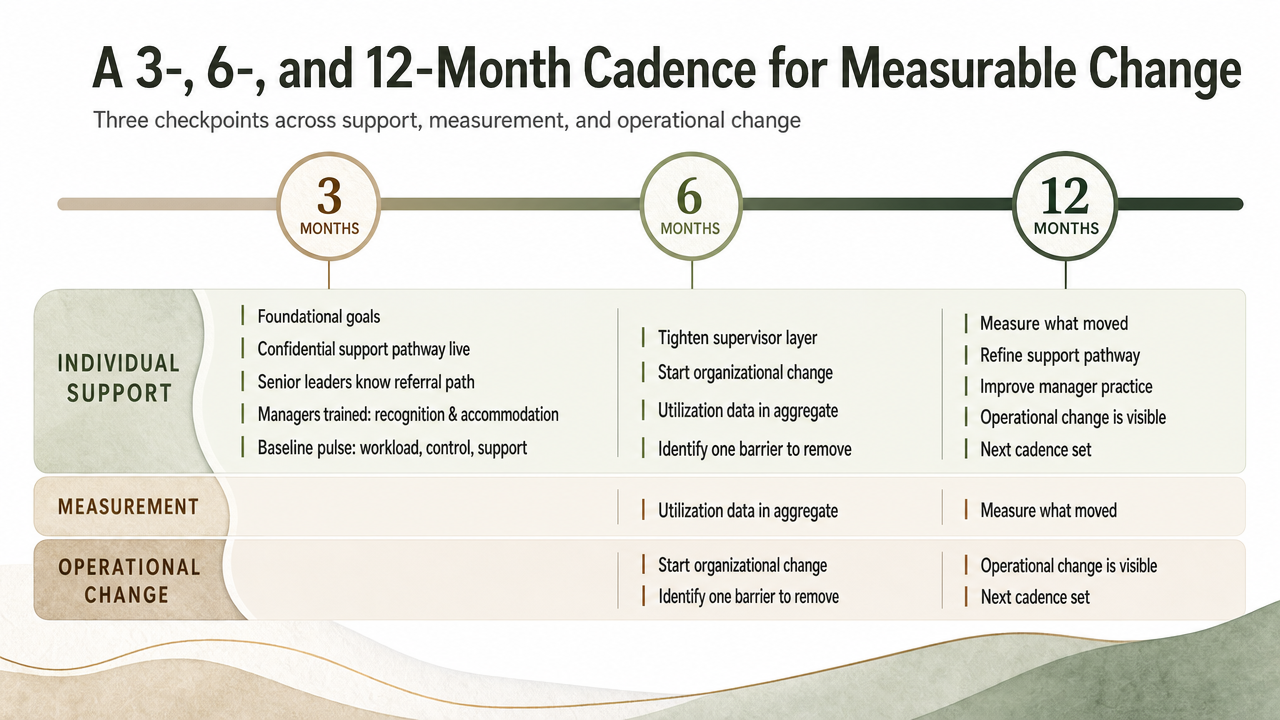
You do not need a five-year roadmap. You need a cadence you can actually run. The CDC's Impact Wellbeing Guide recommends setting 3-, 6-, and 12-month goals across individual support, measurement, and operational change 14. Three checkpoints. That is enough structure to stay honest without turning the program into a second job.
- At three months, the goals are foundational. A confidential support pathway is live and a small circle of senior leaders knows how to refer into it. Managers have had one real training on recognition and accommodation conversations. You have a baseline measurement — a short pulse on workload, control, and support — so you can tell later whether anything moved.
- At six months, you tighten the supervisor layer and start on the organizational one. Utilization data comes back, quietly, in aggregate. You identify one workload or authority issue that keeps surfacing and you commit to actually adjusting it. Not studying it. Adjusting it.
- At twelve months, you re-measure. If burnout indicators have softened and a few senior leaders have used the private pathway without incident, the program is working. If nothing moved, the honest question is which layer got skipped.
Small, sequenced, measurable. That is what durable looks like.
Accommodation as a Retention Lever, Not a Compliance Chore
Most executives think about accommodation the way they think about a fire extinguisher — legally required, hopefully never needed, handled by someone else. That framing is costing you people. The EEOC is explicit that employees with mental health conditions may be entitled to accommodations such as altered work schedules or permission to work from home, as long as the change does not create undue hardship 1. Read that as a retention tool, not a compliance form.
Here is what it looks like in practice. A senior director you have invested a decade in comes to HR and says she is starting outpatient treatment. The reflex in most companies is to route this to legal, generate a paper trail, and manage risk. The result is predictable — she interprets the process as a warning shot, quietly starts a job search, and is gone within the year. You have just paid to lose someone irreplaceable because the accommodation conversation felt like a disciplinary one.
The alternative is not softer. It is more strategic. A shifted schedule during the first ninety days of treatment. A remote day on Thursdays when her group therapy runs late. A quieter Q4 travel calendar. None of these change what she delivers over a year. All of them signal that the organization sees her as a person worth adjusting for, not a liability worth documenting.
Your managers are the hinge point. When a supervisor knows how to open an accommodation conversation without turning it into a legal event — and knows the difference between a request that triggers real obligations and one that just needs a calendar tweak — the disclosure lands differently. The employee stays. The team keeps its leader. The organization keeps the institutional knowledge that took years to build.
Give your senior team the same dignity you would want if the roles were reversed. That is what turns a compliance obligation into the reason your best people stay when the hardest year of their lives happens to overlap with a fiscal quarter.
Choosing a Concierge Partner Without Rebuilding Your Benefits Stack
You do not need to tear up your benefits contracts to add a concierge layer. What you need is a partner that fits into the gap your existing stack cannot fill — the after-hours call, the executive who refuses to use the standard portal, the referral that has to happen in three days instead of three weeks. Everything else stays where it is.
SAMHSA's guidance on selecting workplace behavioral health support is refreshingly plain. Employers should be clear about what they want and can afford, and should ask any prospective partner about fees, qualifications, timelines, and evaluation methods 16. Those four questions do most of the work.
- Fees tell you whether the model scales with your workforce.
- Qualifications tell you whether the clinical bench is real — CIP, CRC, LMHC, LMFT, MSW, licensed psychology — or whether you are buying a call center with a nicer script.
- Timelines tell you whether a senior leader in distress on Tuesday sees someone by Friday.
- Evaluation methods tell you whether you will have anything to show the board in twelve months.
Add three questions of your own.
- How does the partner protect confidentiality when the person calling is a name your HR team would recognize?
- How does the partner coordinate with the clinicians already in your medical network, so an employee does not have to explain their situation twice?
- What does the handoff look like before, during, and after any level of clinical care — the periods where most programs quietly drop the ball?
The right partner does not replace your EAP, your health plan, or the manager training you just funded. It layers on top, catches the people those systems miss, and returns them to the workforce with their dignity and their role intact. That is what you are actually buying — continuity, discretion, and a single phone number your best people will actually pick up. Providers operating from Boca Raton, including teams like Next Level Wellness & Behavioral Health, structure their engagements around exactly that layered model.
The Human Weight of Getting This Right
Underneath the program design, the accommodation language, and the vendor questions, there is a person. A colleague you have worked alongside for years. A leader whose kids you have watched grow up in holiday photos on their desk. When the moment comes — the disclosure, the missed week, the quiet request for help — how your organization responds becomes something that person carries for the rest of their career.
You will not get every one of these moments right. Nobody does. What you can do is build the scaffolding so that when a supervisor freezes, there is a phone number. When a senior leader hesitates, there is a private path. When a team member returns after treatment, there is a role waiting for them and a manager who knows how to welcome them back without making it strange.
That is the whole point of doing this work. Not compliance. Not utilization metrics. The person who stays, the family that stays intact, the career that gets a second chapter. Every small operational win — one supervisor who handled a conversation well, one leader who used the pathway and came back — is worth more than any dashboard number will ever show.
Frequently Asked Questions
How is concierge workplace behavioral health different from our existing EAP?
Your EAP is built for volume and standardized intake. A concierge layer is built for the people who will not use standardized intake — senior leaders, executives, and specialized professionals who need same-week access, verified clinicians, and a single point of contact protecting their calendar and their name. It sits on top of what you already fund, catching the population that avoids the general portal 16.
What kinds of accommodations are executives and senior staff typically entitled to under the ADA?
Under EEOC guidance, employees with mental health conditions may be entitled to accommodations such as altered work schedules or permission to work from home, provided the change does not create undue hardship 1. For senior staff, that often means a shifted travel calendar during treatment, a remote day tied to a therapy appointment, or a quieter quarter — small adjustments that keep valuable people in their roles.
Why don't one-off wellness workshops move the needle on burnout in our workforce?
Because the format cannot outrun the machinery. A 2025 systematic review found that brief workshops had no sustained effects beyond three months, while participatory organizational interventions reduced burnout for at least 12 months 9. A ninety-minute training does not adjust workload, decision authority, or recognition patterns. Those levers live in how work is designed, so a workshop alone gives you a compliance artifact rather than a real outcome.
How do we protect confidentiality when a senior leader needs substance use or mental health support?
Route the disclosure outside routine HR channels. EEOC guidance already requires confidentiality around medical information 1, but the practical protection comes from a discreet pathway — a private phone number, a coordinator who verifies clinicians without generating internal paperwork, and a clear firewall between the support process and performance management. Senior staff use what feels safe. Build the pathway with that reality in mind.
What should we ask a workplace behavioral health partner before signing on?
SAMHSA recommends asking any prospective partner about fees, qualifications, timelines, and evaluation methods 16. Add three of your own: how confidentiality is protected when a caller's name is recognizable, how the partner coordinates with clinicians already in your medical network, and what the handoff looks like before, during, and after clinical care. Those seven questions surface whether you are buying real clinical depth or a nicer script.
How quickly should we expect to see measurable change after launching a program?
The CDC's Impact Wellbeing Guide recommends 3-, 6-, and 12-month goals across individual support, measurement, and operational change 14. At three months, expect a live confidential pathway and manager training. At six, utilization data and one honest workload adjustment. At twelve, softer burnout indicators and a few senior leaders who used the pathway without incident. Durable change is measured in quarters, not weeks.
References
- Depression, PTSD, & Other Mental Health Conditions in the Workplace: Your Legal Rights. https://www.eeoc.gov/laws/guidance/depression-ptsd-other-mental-health-conditions-workplace-your-legal-rights
- Workplace Supported Recovery | Substance Use and Work. https://www.cdc.gov/niosh/substance-use/workplace-supported-recovery/index.html
- State of the U.S. Health Care Workforce, 2024. https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/state-of-the-health-workforce-report-2024.pdf
- Employee Benefits in the United States - March 2024. https://www.bls.gov/news.release/archives/ebs2_09192024.pdf
- Employee Benefits in the United States, March 2024. https://www.bls.gov/ebs/publications/employee-benefits-in-the-united-states-march-2024.htm
- Psychosocial work exposures and health outcomes: a meta-review of 72 literature reviews and IPD-Work Consortium studies. https://pmc.ncbi.nlm.nih.gov/articles/PMC8504166/
- Association Between Workplace Psychosocial Factors and Mental Health Outcomes: A Systematic Review. https://pmc.ncbi.nlm.nih.gov/articles/PMC8122691/
- Work-related psychosocial risk factors for stress-related mental disorders: an updated systematic review and meta-analysis. https://pmc.ncbi.nlm.nih.gov/articles/PMC7337889/
- Effectiveness of Workplace Mental Health Programs in Reducing Occupational Burnout: A Systematic Review. https://pmc.ncbi.nlm.nih.gov/articles/PMC12375206/
- Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. https://pmc.ncbi.nlm.nih.gov/articles/PMC5627926/
- The role of psychosocial working conditions on burnout and its core component emotional exhaustion. https://pmc.ncbi.nlm.nih.gov/articles/PMC4233644/
- An urgent call to address work-related psychosocial hazards and improve worker mental health. https://pmc.ncbi.nlm.nih.gov/articles/PMC11980372/
- CDC Worksite Health ScoreCard Resources for Action. https://www.cdc.gov/workplace-health-promotion/media/pdfs/2024/06/CDC-ScoreCard-Resources-for-Action-508.pdf
- Impact Wellbeing Guide. https://stacks.cdc.gov/view/cdc/150934/cdc_150934_DS1.pdf
- Mental Health, Drug and Alcohol: Support for the Workplace. https://www.samhsa.gov/find-support/how-to-cope/workplace
- Provide Support | SAMHSA. https://www.samhsa.gov/substance-use/drug-free-workplace/employer-resources/toolkit/provide-support
- Implementation of the Crisis Now Model in Palm Beach County. https://discover.pbc.gov/communityservices/BHSUCOD/Documents/Implementation%20of%20the%20Crisis%20Now%20Model_Final%20Report%20(5).pdf
- Supporting Mental Health in the Workplace | NIOSH Science Bulletin. https://www.cdc.gov/niosh/bulletin/2024/mental-health-work.html
- Employee Benefits in the United States – March 2024. https://www.bls.gov/news.release/pdf/ebs2.pdf
- Burnout in the Workplace: A Review of Data and Policy Responses. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6440285/
- Association Between Workplace Psychosocial Factors and Mental Health Outcomes: A Systematic Review. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8122691/
- Burnout and Mental Health Among Executives and Managers: A Systematic Review. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8157473/
A Voice Shaping the Conversation
The topics explored here—change, self-awareness, recovery, and growth—are the same themes Amanda Marino brings to audiences nationwide through speaking engagements and live events.
Known for her appearances on A&E’s Intervention and Digital Addiction, Amanda speaks to organizations, communities, and leadership teams about navigating adversity, embracing vulnerability, and building lives rooted in purpose. Her message resonates far beyond treatment, offering insight that applies to families, professionals, and anyone standing at a crossroads.



Heal on your terms—any time, anywhere.