
Effective Treatment Planning Examples for Complex Needs
Key Takeaways
- Editor's Pick: Integrated care coordination models provide the most robust safety net for high-net-worth clients by ensuring real-time, multidisciplinary collaboration.
- Assessment-driven plans move beyond standardized protocols to uncover the unique biopsychosocial factors driving each individual's needs.
- Flexible, milestone-based frameworks tie support intensity to actual achievements rather than arbitrary calendar dates.
- Continuum-of-care approaches safeguard critical transition periods, reducing the risk of relapse when moving between levels of support.
1. Individualized Assessment-Driven Treatment Planning Examples
In traditional care settings, professionals often encounter the limitations of standardized assessment protocols—the intake forms that capture symptoms but miss the nuances that define each person's path forward. When exploring effective treatment planning examples, assessment-driven care represents a fundamental shift from one-size-fits-all approaches to truly personalized behavioral health support.
Instead of applying standardized protocols, this methodology begins with a comprehensive evaluation of each person's unique circumstances, challenges, and goals. The depth of this initial assessment directly influences the effectiveness of every intervention that follows.
Individuals navigating substance use disorders, mental health challenges, or eating disorders arrive with vastly different histories, support systems, and readiness for change. According to guidelines from the American Society of Addiction Medicine (ASAM), a thorough assessment examines not just presenting symptoms, but also co-occurring conditions, family dynamics, trauma history, and lifestyle factors that may support or hinder recovery.5
This includes trauma-informed screening instruments that identify adverse experiences affecting current functioning, as well as family system mapping to understand relational patterns. This holistic view creates a foundation for interventions that address root causes beyond surface-level behaviors.
"Personalized care plans based on detailed assessments lead to better engagement and sustained outcomes for individuals navigating complex behavioral health challenges."
Translating this comprehensive understanding into actionable care plans requires both clinical expertise and practical flexibility. Research shows that personalized care plans based on detailed assessments lead to better engagement and sustained outcomes. When individuals see their specific needs reflected in their care approach, they are more likely to participate actively in their own wellness journey.
This is particularly crucial for high-need clients who may have experienced multiple treatment episodes without lasting success. Their complexity demands a level of customization that standard programs simply cannot provide. The assessment process itself serves multiple functions beyond information gathering; it establishes rapport and demonstrates that their unique story matters.
Effective assessment-driven planning also accounts for practical realities that influence treatment success. Work commitments, family responsibilities, privacy concerns, and geographic considerations all factor into creating a viable care strategy. For professionals referring high-net-worth or high-profile clients, this attention to lifestyle integration proves essential.

2. Integrated Care Coordination Models
Effective behavioral health support requires seamless collaboration across multiple touchpoints. Integrated care coordination brings together clinical providers, family members, medical professionals, and support specialists into a unified approach that addresses the whole person instead of isolated symptoms.
This model recognizes that recovery and wellness aren't linear processes confined to treatment facilities—they unfold across daily life, requiring real-time communication and adaptive responses. The foundation of integrated coordination lies in establishing clear communication channels among all stakeholders.
When therapists, prescribing physicians, case managers, and support companions operate from shared information, they can identify emerging challenges before they escalate. Research from Harvard Medical School shows that coordinated care models reduce crisis interventions by ensuring everyone involved understands current goals, medication changes, and environmental factors affecting progress.9
Consider a situation many referring professionals have encountered: a psychiatrist adjusts medication dosages based on reported anxiety symptoms, but the therapist attributes subsequent emotional flatness to therapeutic resistance rather than pharmaceutical side effects. This communication gap can derail weeks of progress.
The integrated coordination model prevents such breakdowns through regular interdisciplinary check-ins where team members share observations and adjust strategies collectively. A companion might notice sleep pattern changes that inform the prescriber's medication review, creating a continuous feedback loop that catches subtle warning signs.
Geographic flexibility represents another crucial dimension of integrated coordination. Professionals working with high-net-worth or high-need clients understand that care cannot pause when someone travels for business or family obligations. Coordinated models maintain continuity across locations by ensuring support resources remain available regardless of time zones or settings.
3. Flexible Milestone-Based Frameworks
Effective coordination between providers creates the infrastructure for tracking meaningful progress across all aspects of care. Milestone-based frameworks build on this foundation by tying support intensity to actual achievements instead of calendar dates.
This approach recognizes that wellness journeys unfold at different paces, with some individuals needing extended support in certain areas while advancing quickly in others. These frameworks establish clear benchmarks that mark meaningful progress.
- Consistent medication adherence and management
- Stable housing and daily routine establishment
- Return to professional or executive responsibilities
- Rebuilding and maintaining healthy family relationships
The individualized assessment process determines which milestones are appropriate for each person's situation, ensuring benchmarks align with their specific needs and circumstances. Organizations like The Joint Commission emphasize that responsive models lead to better long-term outcomes because they meet people where they are instead of forcing them into predetermined boxes.4
The beauty of milestone-based systems lies in their transparency. Everyone involved—the individual receiving support, their family, and the care team—understands exactly what success looks like at each stage. For instance, a milestone might involve attending three consecutive weekly therapy sessions without crisis intervention, demonstrating both commitment and stability.
Flexibility becomes particularly valuable when unexpected challenges emerge. Life doesn't pause for recovery, and milestone frameworks can accommodate real-world complications without derailing progress entirely. If someone faces a major stressor, support can intensify temporarily without restarting the entire process.
Professional teams appreciate how these frameworks facilitate clearer communication with referring providers. Instead of vague progress reports, updates can reference specific milestones achieved or in progress. This concrete language helps everyone assess whether interventions are working and when adjustments might be needed.
4. Continuum-of-Care Treatment Planning Examples
Effective behavioral health support requires thinking beyond isolated treatment episodes. While milestone-based frameworks help identify when someone is ready to progress, continuum-of-care planning addresses what happens between those milestones—the transitions, adjustments, and inevitable challenges that arise as needs evolve.
This approach recognizes that milestones mark transition points between phases of care, and it is often in these in-between spaces where individuals need the most thoughtful support. Most referring professionals have seen the pattern: a client completes residential treatment, reaches important milestones, and appears ready for the next phase—then struggles during the transition itself.
The continuum framework addresses this by planning for interconnected phases, ensuring individuals have access to the right intensity of care at the right moment. Rather than treating these as separate episodes, effective planning focuses on the handoffs between phases and the support needed during each transition.
Modern care teams often utilize secure digital platforms where a simple Status Update or entering phase_transition_metrics can instantly align the entire multidisciplinary team. The transitional support phase deserves particular attention because it is where many well-planned care strategies falter.
Consider the common scenario of someone leaving residential care: they have completed treatment, demonstrated progress, and are ready to return home. Then comes that critical 30-day window after discharge. Data from the Substance Abuse and Mental Health Services Administration (SAMHSA) consistently shows this transitional period carries heightened risk, yet it is often when formal support decreases most dramatically.1
Continuum planning addresses this gap by maintaining flexible, responsive support during transitions—perhaps through daily check-ins that gradually decrease, readily available crisis support, or hands-on assistance establishing new routines. The goal is ensuring someone has access to the right intensity of care at the right moment, rather than facing an abrupt shift from high structure to independence.
What makes continuum-of-care planning particularly valuable for complex cases is its built-in adaptability. Movement between phases isn't always linear—someone might need to temporarily increase support intensity during a life transition, family crisis, or unexpected stressor.
Insight Beyond Treatment
At Next Level Wellness & Behavioral Health, we believe meaningful change starts with perspective, not just protocols.
That philosophy is directly led by Amanda Marino, whose voice in behavioral health extends beyond clinical settings into leadership, culture, and personal growth.
Through keynote speaking and live events, Amanda explores the deeper themes that show up in recovery, family systems, and life transitions: authenticity, resilience, accountability, and the courage to change. Her work invites audiences to move past labels and into honest conversations that create lasting impact.

Partnering for Complex Care Solutions
The four planning approaches explored throughout this article—assessment-driven, coordinated, milestone-based, and continuum care—each address distinct client needs. Yet some cases require integration across multiple approaches simultaneously.
When clients present with co-occurring disorders alongside family system challenges, or when geographic distance complicates coordination across treatment modalities, a single planning framework rarely suffices. These complex situations call for collaborative partnerships that weave together different planning strategies into a cohesive support structure.
Why is multidisciplinary partnership crucial for high-net-worth clients?
High-net-worth individuals often face unique pressures, including public scrutiny, demanding executive schedules, and complex family estates. A multidisciplinary partnership ensures that clinical, lifestyle, and privacy needs are managed simultaneously without compromising the quality of care or discretion.
Professional collaboration in these contexts means creating integrated care teams where each provider contributes specialized expertise while maintaining shared accountability for outcomes. One team member might lead clinical treatment using assessment-driven protocols, while another coordinates family dynamics and daily living support through milestone-based tracking.
A third might manage the continuum of care transitions as clients move between treatment phases. This isn't about dividing a client into separate problems—it's about surrounding them with complementary expertise that addresses their situation holistically.
Consider a client transitioning from residential treatment with both substance use and eating disorder histories, returning to a family system with its own unresolved dynamics, while managing a high-profile career that demands discretion. This scenario requires coordinated planning across clinical treatment, nutritional support, family therapy, and workplace reintegration.
Effective partnerships establish clear role delineation from the outset while building communication protocols that keep everyone aligned. Shared documentation systems, scheduled case conferences, and agreed-upon decision-making processes prevent the fragmentation that often derails complex cases.
When referring professionals encounter cases that exceed single-provider capacity, early recognition makes the difference between sustainable progress and cycling through fragmented services. These situations benefit from teams that understand how different planning approaches complement each other and can adapt their coordination as client needs evolve.
For support that meets you right where you are—anytime, anywhere—connect with us today.
Frequently Asked Questions
How were these treatment planning examples selected for complex needs?
These treatment planning examples were selected based on their direct alignment with evidence-based standards and their proven effectiveness for clients with complex or co-occurring needs. Industry leaders rely on recommendations from organizations such as SAMHSA, ASAM, and The Joint Commission, which emphasize individualized, multidisciplinary, and flexible planning approaches. Peer-reviewed research was reviewed to ensure each example supports real-world outcomes—like improved engagement, reduced readmission, and long-term recovery. Only practices supported by clinical guidelines and validated in high-acuity environments were included, ensuring relevance for professionals managing complex cases.3
What makes assessment-driven planning particularly effective for high-complexity clients?
Assessment-driven planning stands out for high-complexity clients because it focuses on the unique interplay of medical, psychiatric, social, and lifestyle factors that shape each case. By grounding treatment plans in comprehensive biopsychosocial evaluations, clinical teams can identify co-occurring disorders, social determinants, and readiness to change—building a foundation for truly individualized care. Research shows this approach leads to more accurate placements and better recovery outcomes, especially when compared to generic or symptom-focused models. For professionals managing complex needs, these treatment planning examples ensure that no critical detail is overlooked and care remains adaptable as new information emerges.5
How do integrated care coordination models differ from traditional referral networks?
Integrated care coordination models set themselves apart from traditional referral networks by fostering real-time collaboration, shared decision-making, and proactive communication among all providers. Instead of passing clients from one specialist to the next, these models encourage multidisciplinary team meetings, centralized case management, and the use of secure digital platforms for information exchange. Research from Harvard Medical School highlights that integrated coordination reduces care fragmentation and leads to better outcomes for individuals with complex needs. While referral networks focus on connecting clients to resources, integrated models ensure everyone stays aligned on goals, progress, and changes—making treatment planning examples more seamless and client-centered.9
Why aren't protocol-based treatment plans included in these examples?
Protocol-based treatment plans are intentionally excluded from these treatment planning examples because they often lack the flexibility required for clients with complex or co-occurring needs. Strict, one-size-fits-all protocols may overlook key factors like co-existing mental health conditions, family dynamics, or unique lifestyle demands. Industry guidelines from experts such as SAMHSA and The Joint Commission emphasize the importance of individualized, adaptive planning to achieve meaningful outcomes for high-acuity populations. In practice, customized plans allow clinical teams to respond dynamically as new information or challenges arise, supporting better long-term recovery and engagement.1,4
What role does technology play in modern treatment planning for complex cases?
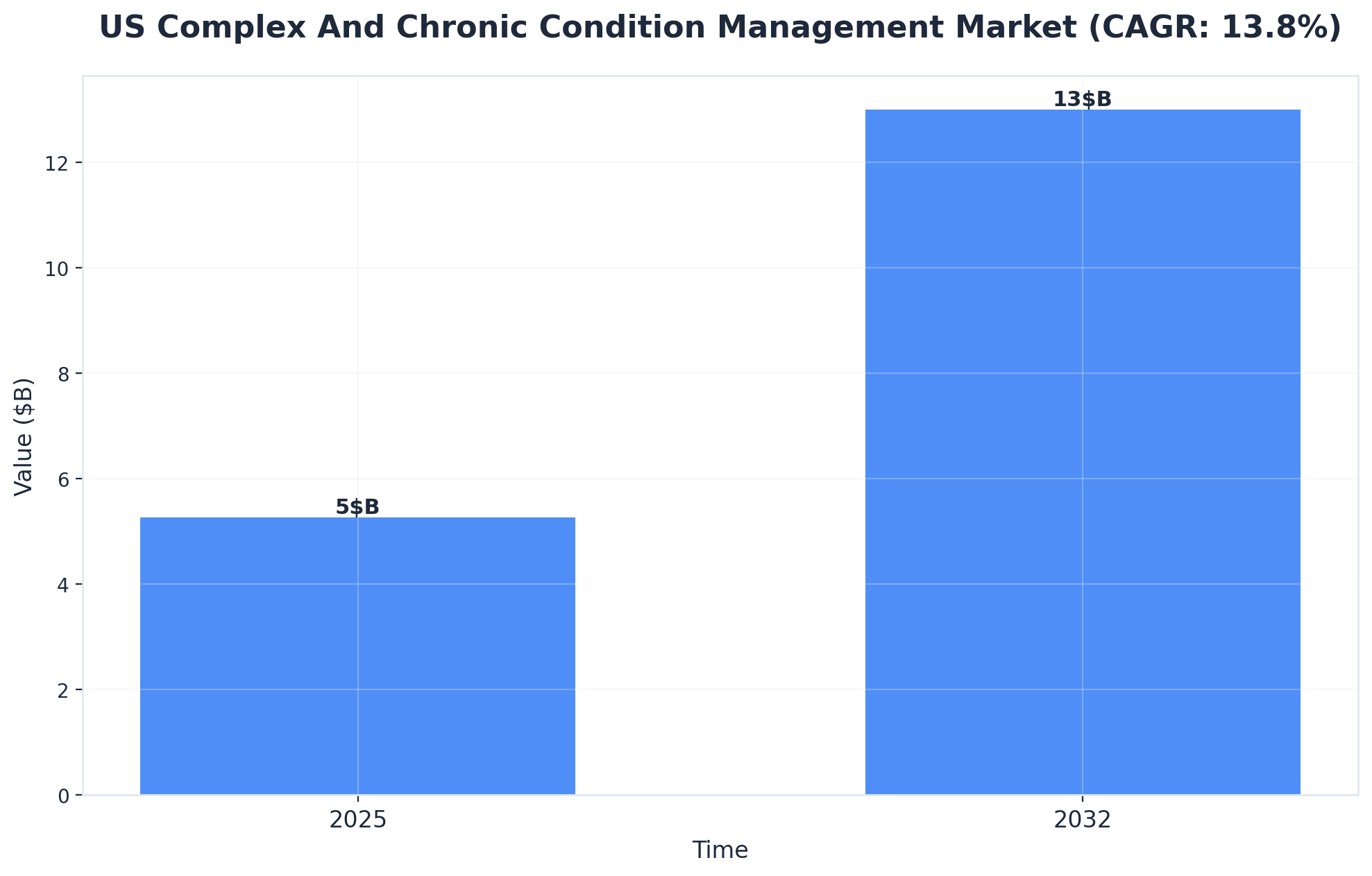
Technology is now a cornerstone of effective treatment planning for complex cases, helping clinical teams coordinate, monitor, and adapt care in real time. Digital care platforms enable secure sharing of progress notes, lab data, and scheduling among multidisciplinary providers, which reduces communication gaps and boosts efficiency. Artificial intelligence and decision support tools are also emerging, offering predictive analytics for risk assessment and individualized care pathways. Industry analysts note that the treatment planning systems market is growing rapidly, fueled by advancements in AI and increasing demand for integrated digital solutions. For professionals managing high-acuity clients, technology ensures that treatment planning examples remain adaptive, data-driven, and client-centered.4
How do you measure treatment plan effectiveness for clients with co-occurring disorders?
Measuring treatment plan effectiveness for clients with co-occurring disorders relies on tracking both clinical outcomes and functional improvements over time. Key indicators include reduced symptom severity, improved medication adherence, and enhanced daily functioning—like stable housing, employment, or healthier relationships. Industry leaders find that regular progress reviews, client self-reports, and family feedback help capture changes that matter most in real life. Standardized tools, such as those recommended by The Joint Commission, support objective measurement and promote consistency across care teams. Treatment planning examples that use these multidimensional assessments help ensure plans remain effective and responsive to evolving needs.4
What documentation standards should treatment plans meet for professional collaboration?
Treatment plans shared among professionals must meet standards that ensure clarity, accountability, and legal compliance. Documentation should be detailed, timely, and structured—including clear goals, interventions, progress notes, and measurable outcomes. Leading organizations such as The Joint Commission stress that plans must also record client consent, risk assessments, and coordination steps to support safe, collaborative care. Consistent use of standardized forms and secure digital platforms helps minimize miscommunication and facilitates seamless transitions. When reviewing treatment planning examples, professionals should confirm that documentation supports multidisciplinary teamwork and meets industry requirements for privacy and auditability.4
References
- SAMHSA (Substance Abuse and Mental Health Services Administration). https://www.samhsa.gov/
- NIDA (National Institute on Drug Abuse). https://www.nida.nih.gov/
- NIH/NLM PubMed Central. https://www.ncbi.nlm.nih.gov/pmc/
- The Joint Commission. https://www.jointcommission.org/
- ASAM (American Society of Addiction Medicine). https://www.asam.org/
- American Psychological Association (APA). https://www.apa.org/
- CARF International. https://www.carf.org/
- Cochrane Collaboration. https://www.cochrane.org/
- Harvard Medical School. https://hms.harvard.edu/
- Johns Hopkins Medicine - Department of Psychiatry and Behavioral Sciences. https://www.hopkinsmedicine.org/psychiatry/
A Voice Shaping the Conversation
The topics explored here—change, self-awareness, recovery, and growth—are the same themes Amanda Marino brings to audiences nationwide through speaking engagements and live events.
Known for her appearances on A&E’s Intervention and Digital Addiction, Amanda speaks to organizations, communities, and leadership teams about navigating adversity, embracing vulnerability, and building lives rooted in purpose. Her message resonates far beyond treatment, offering insight that applies to families, professionals, and anyone standing at a crossroads.



Heal on your terms—any time, anywhere.