
Building a Recovery Plan with a Clinical Interventionist

Executive Summary: Strategic Recovery Planning
For families managing complex behavioral health crises, professional coordination is the differentiator between temporary fixes and sustainable outcomes. Here are the critical success factors:
- Concurrent Care is Non-Negotiable: Treating mental health and substance use sequentially increases relapse risk; integrated models are the clinical standard.
- Mobilize Recovery Capital: Success depends on addressing Social Determinants of Health (SDOH)—housing, employment, and community connection—alongside medical care.
- Collaborative Engagement: Invitational models (like ARISE®) yield 96% treatment entry rates within six months by reducing resistance and aligning family systems.
Immediate Action: If your current plan does not account for all six ASAM dimensions listed below, request a comprehensive re-assessment immediately.
How a Clinical Interventionist Ensures a Clinically Sound Plan
Six Assessment Dimensions Guiding Care
To create a truly effective recovery plan, a clinical interventionist utilizes a multidimensional assessment tool that examines six key areas of a person’s life. For professionals, the ASAM Criteria offers the industry standard: it organizes care around these six assessment dimensions to ensure no key factor is overlooked.
This comprehensive checklist guides the process, ensuring that medical, psychological, and environmental factors are weighed equally:
- Dimension 1: Acute intoxication and withdrawal potential
- Dimension 2: Biomedical conditions and complications
- Dimension 3: Emotional, behavioral, or cognitive conditions
- Dimension 4: Readiness to change
- Dimension 5: Relapse, continued use, or continued problem potential
- Dimension 6: Recovery and living environment
Each dimension plays a unique role in the strategic planning of care. For example, evaluating withdrawal risk (Dimension 1) may determine if immediate medical supervision is necessary, while Dimension 6 looks at how housing, family, and social context will affect long-term outcomes. This approach works best when treatment complexity is high—such as with co-occurring mental health and substance use concerns—or when social factors might cause relapse if left unaddressed.
Research shows that care grounded in these six dimensions leads to more appropriate placement, improved engagement, and better sustained recovery rates. This method also supports person-centered planning, helping teams set realistic goals and adapt as circumstances change.1
Evidence-Based vs. Generalized Approaches
A common debate among behavioral health professionals centers on whether to ground recovery plans in evidence-based practices or rely on more generalized, one-size-fits-all approaches. At its core, "evidence-based" means that the interventions and strategies used have been rigorously tested and proven effective through scientific research, rather than being based solely on tradition or personal experience.
A clinical interventionist is trained to prioritize evidence-based planning. The table below outlines the strategic differences between these two methodologies for decision-makers:
Industry findings reveal that individuals are significantly more likely to achieve their treatment goals and maintain recovery when their care plan is matched to interventions supported by research, rather than generic programming. Generalized approaches might appeal where resources or access to specialized training are limited, but research consistently demonstrates that personalized, research-backed plans outperform these models in both engagement and results.5
Integrated Treatment for Co-Occurring Needs
Why Concurrent Care Outperforms Sequential
A practical decision tool for professionals: If both mental health and substance use conditions are present, use this quick assessment logic to determine the care path. If treating one without the other risks undermining overall progress, concurrent care is the priority.
Research consistently supports integrated treatment as the superior approach for co-occurring needs. Sequential models, where one disorder is addressed before the other, often leave underlying symptoms untreated, resulting in higher relapse rates and less sustainable outcomes. In contrast, concurrent care brings both conditions into focus simultaneously, improving engagement and producing more durable recovery gains.
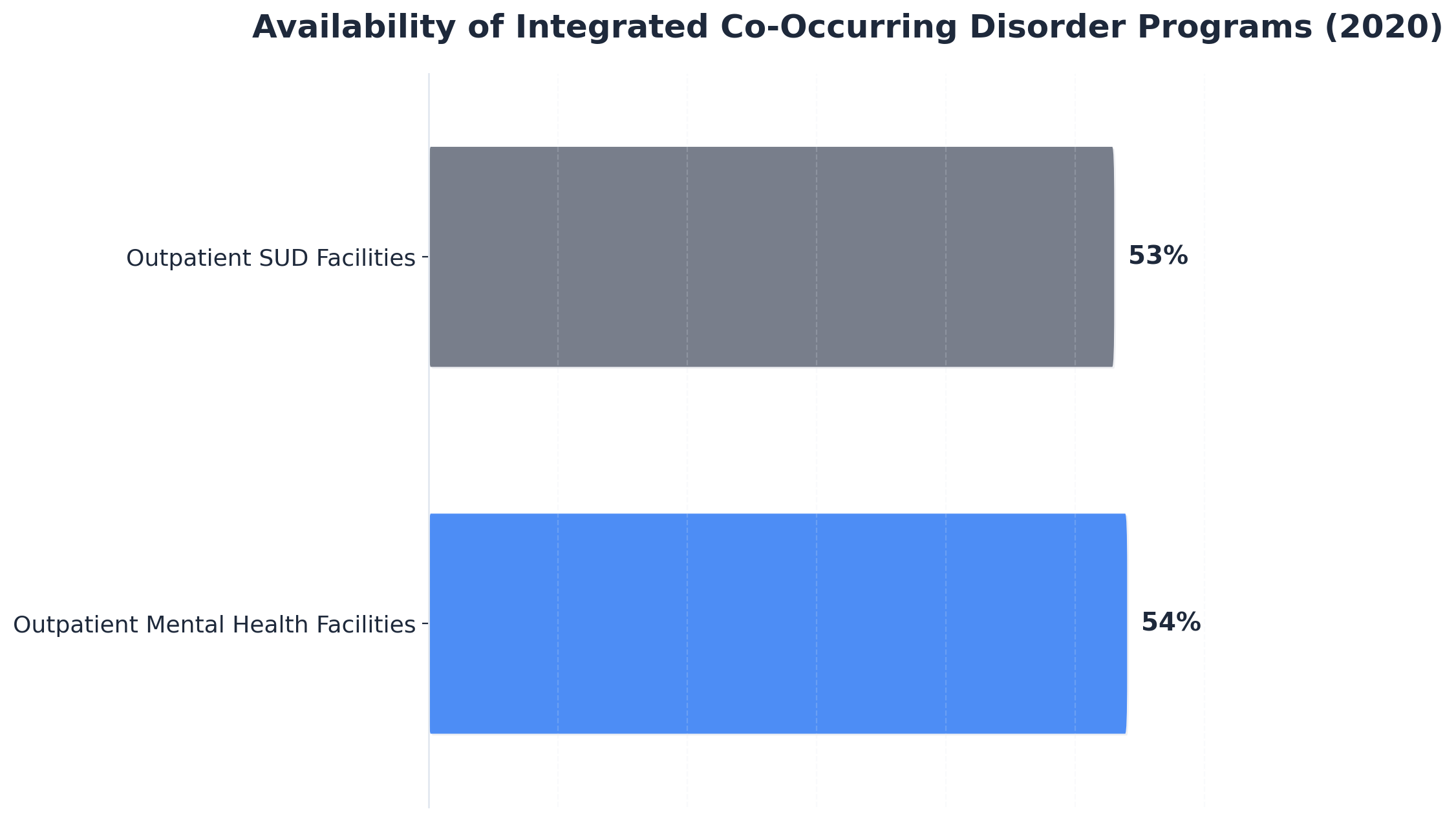
A clinical interventionist will often collaborate with a multidisciplinary team to implement concurrent care, meaning psychiatrists, therapists, and case managers all work together under a unified plan. Studies reveal that integrated models are now considered the standard of care, with over half of outpatient mental health and substance use disorder facilities offering specialized co-occurring disorder programs as of 2020—a marked increase from past years.9
Trauma-Informed Planning Essentials
Trauma, defined as any deeply distressing or disturbing experience, often shapes both mental health and substance use patterns. A trauma-informed recovery plan starts with a practical checklist to ensure safety and efficacy:
- Screen for History: Systematically identify past trauma history without forcing disclosure.
- Identify Symptoms: Recognize trauma-related symptoms that may mimic or exacerbate other conditions.
- Integrate Safety: Implement specific trust-building measures and emotional safety protocols.
- Collaborate: Involve the person in every step of planning to restore agency.
- Prevent Re-traumatization: Select interventions that avoid triggering past traumatic events.
A clinical interventionist brings a trauma-informed lens to the table by realizing how prevalent trauma is, recognizing its impact on behaviors and relationships, and responding with practical, empowering support. This method works when clients present with complex or unclear histories, or when previous treatment attempts have failed due to unresolved trauma.
For organizations, this approach fits teams aiming to improve engagement and reduce treatment drop-out rates, especially in populations with high rates of childhood adversity or interpersonal violence. Research shows that when trauma is addressed systematically, outcomes improve—clients are more likely to remain in care and progress toward their goals.6
Insight Beyond Treatment
At Next Level Wellness & Behavioral Health, we believe meaningful change starts with perspective, not just protocols.
That philosophy is directly led by Amanda Marino, whose voice in behavioral health extends beyond clinical settings into leadership, culture, and personal growth.
Through keynote speaking and live events, Amanda explores the deeper themes that show up in recovery, family systems, and life transitions: authenticity, resilience, accountability, and the courage to change. Her work invites audiences to move past labels and into honest conversations that create lasting impact.

Mobilizing Recovery Capital: The Clinical Interventionist Role
Social Determinants in Treatment Success
In behavioral health, Social Determinants of Health (SDOH) refer to the nonmedical factors—like where someone lives, works, and connects socially—that shape recovery outcomes. Recent research highlights that these factors can have a greater effect on health and recovery than genetics or access to healthcare alone.8
SDOH Screening Checklist for Recovery Planning:
- Housing Status: Is the living environment stable and sober-safe?
- Employment/Education: Does the client have access to vocational or educational purpose?
- Transportation: Are there reliable means to attend treatment and support groups?
- Food Security: Are basic nutritional needs being met consistently?
- Social Support: Is there a network of non-using peers and community connections?
A clinical interventionist integrates SDOH screening into recovery planning, collaborating with multidisciplinary teams to ensure barriers like unstable housing or job insecurity are addressed. This path makes sense for professionals supporting individuals whose recovery is complicated by financial stress, lack of support, or community disconnection. Studies show that interventions focused on SDOH domains—especially healthcare system navigation and community context—lead to improved treatment initiation, reduced substance use, and less stigma in opioid use disorder care.10
Case Management and Coordination Functions
In the behavioral health field, case management refers to organizing and monitoring all the services and supports a person needs for recovery, from treatment planning to resource linkage and ongoing advocacy. A clinical interventionist often acts as the central coordinator, keeping everyone aligned and moving toward shared goals.
"Effective case management bridges the gaps between fragmented services, improves treatment retention, and reinforces recovery goals throughout the continuum of care."3
A practical case management tool for professionals involves mapping out each client’s network of resources, assigning clear responsibilities to care team members, and setting up regular progress check-ins. This structure ensures that support—whether for housing, mental health, medical needs, or employment—remains coordinated and responsive.
For teams aiming to operationalize recovery capital—from housing and healthcare navigation to employment and peer support—robust case management is essential. Opt for this framework when long-term engagement and cross-disciplinary collaboration are priorities.
From Intervention to Sustained Engagement
Collaborative Models and Treatment Entry
Collaborative models, where families, clinicians, and the individual work together, have been shown to dramatically increase the likelihood of successful treatment entry. The clinical interventionist often leads these efforts, facilitating open dialogue and ensuring the plan aligns with the client’s readiness and personal values.
View ARISE® Model Success Statistics
Recent studies highlight that the ARISE® Comprehensive Care model, which emphasizes collaboration over confrontation, results in:3,4
- >60% of individuals entering treatment within one week.
- 83% entering within three weeks.
- 96% entering within six months.
A practical engagement tool for professionals involves creating a shared roadmap with clients and their support networks. This outlines each step from initial engagement to treatment entry, clarifies everyone’s role, and sets clear expectations for communication and follow-up. This approach works best when families are available and willing to participate, or when previous attempts at solo intervention have fallen short.
Peer Support and Aftercare Integration
Peer support—meaning guidance from those with lived recovery experience—has emerged as an evidence-based pillar in sustaining engagement after formal treatment ends. A clinical interventionist typically coordinates these supports, ensuring a seamless handoff between clinical and community resources.
A practical tool for aftercare planning involves mapping out a layered support system:
- Peer Recovery Coaching: One-on-one mentorship for daily accountability.
- Alumni Connections: Integration into a community of shared experience.
- Structured Check-ins: Scheduled touchpoints to monitor progress.
- Referral Networks: Immediate access to local or virtual support groups.
Studies confirm that integrating peer recovery services with clinical care improves both treatment linkage and ongoing participation, particularly for clients transitioning out of intensive settings. Aftercare integration goes beyond referrals—it’s about embedding ongoing connection and accountability into the recovery plan.7

Experience the Difference of Concierge, Coordinated Support
This is where 24-hour companions, coordinated care teams, and global mobilization capacity make the difference between reactive scrambling and purposeful progress. The final week emphasizes transition planning, whether that involves stepping down care levels, adjusting support structures, or preparing for the next recovery phase. Our intervention specialists and case managers coordinate every detail—from prescription management to post-treatment companion support—ensuring nothing falls through the cracks.
When your child's crisis demands immediate action, the next 30 days require professional orchestration, not guesswork. You understand the clinical complexities at play—now you need expert coordination to execute what you already know must happen. Our case managers and intervention specialists transform this critical month from overwhelming chaos into a structured roadmap, handling the logistics while you focus on your family.
Let's Create Lasting Change, Together
At Next Level Wellness & Behavioral Health, we provide premier concierge behavioral healthcare and highly personalized support for individuals and families navigating substance use, mental health challenges, eating disorders, complex life transitions, and more.
Our discreet, concierge, and expert-driven approach ensures dignity, compassion, and results-oriented care whether at home, in transit, or across multiple levels of treatment.
For support that meets you right where you are—anytime, anywhere—connect with us today.
Frequently Asked Questions
How do I choose between invitational and traditional intervention models?
Choosing between invitational and traditional intervention models depends on client and family dynamics. Invitational approaches, such as ARISE®, emphasize transparency and collaboration, inviting the individual and their support system into the process from the start. Studies show these models result in higher rates of treatment entry—over 60% within one week and 96% within six months—largely because they minimize resistance and foster trust. Traditional (often confrontational) models may be considered if safety or imminent harm is a concern and prior collaborative efforts have failed. A clinical interventionist will assess readiness, risk, and family willingness to help identify the best fit for each situation.3,4
What's the typical timeline from initial assessment to treatment entry?
The typical timeline from initial assessment to treatment entry with a clinical interventionist can be surprisingly swift, especially when collaborative models are used. Studies show that over 60% of individuals enter treatment within one week after the first assessment and intervention meeting, with 83% entering within three weeks and 96% within six months. This rapid progression is most likely when families and support networks are actively involved and communication between all parties is clear. If complex barriers—like housing or medical needs—are present, the process may take longer, but most cases move forward within days to weeks rather than months.3,4
How does a clinical interventionist coordinate with existing healthcare providers?
A clinical interventionist coordinates with existing healthcare providers by acting as a central communicator and care organizer. This usually involves gathering input from physicians, therapists, and case managers, then developing a unified plan that addresses all aspects of the client’s needs. The interventionist facilitates regular team meetings, updates on progress, and ensures all providers are aligned on treatment goals and interventions. This approach is ideal for complex cases involving multiple specialties or frequent transitions between levels of care. Research highlights that effective case management and coordination reduce service fragmentation and improve treatment retention and outcomes.3
What happens when housing or employment barriers complicate treatment planning?
When barriers like unstable housing or job loss complicate treatment planning, a clinical interventionist addresses these social determinants of health directly in the recovery plan. This might involve connecting the individual with supportive housing programs, employment resources, or community-based services—since research shows these factors can influence recovery as much as medical care itself. For professionals, case management becomes essential: mapping out resource needs, coordinating with agencies, and advocating for access all help keep the recovery plan on track. Studies confirm that interventions targeting housing and employment lead to better treatment engagement and reduced relapse risk.8,10
How is readiness for change assessed when someone doesn't acknowledge the problem?
When a person doesn’t acknowledge the problem, a clinical interventionist uses validated tools—often motivational interviewing and structured readiness assessments—to gauge their stage of change. This means listening for language that signals willingness, resistance, or ambivalence, rather than demanding immediate agreement. Research shows that assessing readiness is essential for tailoring interventions and involves exploring the individual’s values, goals, and perceived barriers. If someone is precontemplative (not yet recognizing a need to change), the interventionist focuses on building rapport and gently increasing awareness, rather than pushing for action. This approach allows the team to meet clients where they are and adapt strategies accordingly.2
What role does family involvement play in clinical intervention outcomes?
Family involvement plays a critical role in the success of clinical intervention outcomes. When families actively participate alongside a clinical interventionist, research shows treatment entry rates rise dramatically—over 60% within the first week and up to 96% within six months using collaborative models like ARISE®. Family support helps reduce resistance, foster trust, and create a network of accountability that sustains engagement even through setbacks. This approach works particularly well when families are willing to engage, as it aligns everyone around shared goals and provides consistent encouragement. For clinical teams, facilitating family involvement means more stable transitions and stronger long-term recovery outcomes.3,4
References
- The ASAM Criteria, Fourth Edition. https://www.asam.org/asam-criteria
- Substance Abuse Treatment Planning. https://www.ncbi.nlm.nih.gov/books/NBK572945/
- TIP 27: Comprehensive Case Management for Substance Abuse Treatment. https://library.samhsa.gov/sites/default/files/sma15-4215.pdf
- Integrating Treatment for Co-Occurring Mental Health Conditions. https://pmc.ncbi.nlm.nih.gov/articles/PMC6799972/
- What Is Evidence-Based Practice?. https://www.abct.org/get-help/what-is-evidence-based-practice/
- Trauma-Informed Care: A Sociocultural Perspective. https://www.ncbi.nlm.nih.gov/books/NBK207195/
- Peer Recovery Support Services and Recovery Coaching for Substance Use Disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC12811009/
- Social Determinants of Health (SDOH) | About CDC. https://www.cdc.gov/about/priorities/why-is-addressing-sdoh-important.html
- Availability and Correlates of Integrated Treatment for People with Co-Occurring Disorders. https://aspe.hhs.gov/reports/availability-correlates-integrated-treatment-people-cods
- A Scoping Review of Interventions Addressing Social Determinants of Health in Opioid Use Disorder. https://pmc.ncbi.nlm.nih.gov/articles/PMC12684375/
- SAMHSA National Helpline. https://www.samhsa.gov/find-help/national-helpline
- 988 Suicide & Crisis Lifeline. https://988lifeline.org/
- SAMHSA's FindTreatment.gov. https://www.findtreatment.gov/
- NAMI (National Alliance on Mental Illness). https://www.nami.org
A Voice Shaping the Conversation
The topics explored here—change, self-awareness, recovery, and growth—are the same themes Amanda Marino brings to audiences nationwide through speaking engagements and live events.
Known for her appearances on A&E’s Intervention and Digital Addiction, Amanda speaks to organizations, communities, and leadership teams about navigating adversity, embracing vulnerability, and building lives rooted in purpose. Her message resonates far beyond treatment, offering insight that applies to families, professionals, and anyone standing at a crossroads.



Heal on your terms—any time, anywhere.