
7 Questions to Find the Right Alcohol Treatment Near Me

Key Takeaways
- Ask which evidence-based therapies clinicians deliver by name, like CBT or motivational enhancement, because vague terms like 'holistic' signal marketing rather than structured clinical care.13
- Confirm the specific clinician you will work with and their credentials, since continuity with one licensed, addiction-trained provider matters more than the program's brand.10
- Ask whether the program prescribes naltrexone, acamprosate, or disulfiram in-house, since these FDA-approved medications are underused but supported as legitimate first-line options.4,15
- Insist on integrated care for anxiety, depression, or trauma alongside drinking, because sequencing the drinking first rarely works when co-occurring conditions drive use.9
- Push on schedule, telehealth, and privacy options, and expect a quality program to recommend the lowest level of care that safely treats you.1,8
- Ask what the program actually measures, like attendance, craving scores, and drinking events, since programs that track outcomes produce better engagement and retention.5
- Get specific numbers on length of care, total cost, insurance status, and self-pay options so you can compare programs apples to apples rather than by sticker price.7
Why "near me" is the wrong starting point
You typed those three words into a search bar at some point this week. Maybe at 11 p.m. after a long day, maybe between meetings, maybe in a hotel room. The proximity instinct makes sense. You want this handled quickly, quietly, and on your own terms.
Here is the problem with proximity as your first filter: the closest program may not deliver care that matches what you actually need, and the most advertised one may not be the highest quality. Millions of adults in the U.S. meet criteria for alcohol use disorder in a given year, which means the market is large enough to include everything from clinician-led outpatient practices to glossy 30-day brochures that mostly sell a setting.16
The better starting question is fit. A high-quality alcohol treatment provider can answer specific questions about the therapies they use, the credentials of their clinicians, whether they prescribe medication, and how they coordinate care for anxiety, depression, or trauma alongside drinking. The NIAAA Alcohol Treatment Navigator was built precisely so people like you could compare programs on quality, not marketing.2,13
And "near me" has quietly widened. Since 2020, far more providers deliver alcohol care through telehealth, including accredited fully virtual programs. A clinician three time zones away may be a closer fit than the building down the block. The seven questions ahead will help you tell the difference.1
How to use the seven questions on an intake call
Block 20 minutes. Not five. Not "between things." A real intake conversation with a quality program runs longer than you expect, and the ones that try to rush you off the phone tell you something useful about how they treat clients.18
Open with a single sentence about your situation and what you need from care. You do not owe a stranger your full history on a first call. "I'm a working professional looking for outpatient or telehealth options that protect my schedule and my privacy" is enough to set the frame.
Then ask the seven questions in order. Write down the answers, even shorthand. The NIAAA Navigator suggests keeping a simple comparison sheet across providers, because by call three you will not remember which program said what. Listen for specifics: named therapies, named credentials, named medications, named timelines. Vague reassurance is a red flag.10
If an answer is thin, ask one follow-up, then move on. You are not negotiating. You are gathering data on which clinician earns the next conversation.
The seven questions that separate concierge-grade care from a brochure
Question 1: Which evidence-based therapies do your clinicians actually deliver?
Ask it that way. Not "do you use evidence-based therapies" — every program will say yes. Ask which ones, by name, and which clinician on staff is trained to deliver each.
The NIAAA Navigator considers a strong answer to include specific named therapies: cognitive behavioral therapy, motivational enhancement therapy, and structured behavioral approaches built around relapse prevention. A weak answer sounds like "holistic," "integrative," or "customized to you" with no clinical noun attached. Holistic is not a therapy. It is a marketing word.13
Follow up by asking how the therapy is actually delivered week to week. A real CBT protocol involves homework, between-session practice, and measurable targets. If the program describes therapy as open-ended conversation that "goes where you need it to go," that may still be valuable, but it is not what the research literature means by evidence-based care.18
For a working professional, there is a practical reason to push on this. Structured therapies have a defined arc. You can plan around 12 to 16 weeks of weekly sessions in a way you cannot plan around an indefinite supportive process. That predictability matters when you are also planning around a trial calendar, a fundraise, or a hospital schedule.
If the person on the phone cannot name two specific therapies and the credential of the clinician who delivers each, end the call politely and try the next provider on your list.
Question 2: Who will I work with, and what are their credentials?
You are not hiring a building. You are hiring a person, or a small team. Ask who that will be.
A quality program can tell you, before you sign anything, the credentials of the primary therapist you would be assigned to and the prescriber you would see if medication came up. Listen for licensed clinical credentials: LCSW, LMFT, LMHC, licensed psychologist, board-certified addiction medicine physician, or psychiatric nurse practitioner with addiction training. Listen for addiction-specific certification on top of the base license — formal training in alcohol use disorder, not just general counseling experience.8,10
A weak answer assigns you to "the team" or "whoever is available." A strong answer names the clinician, describes their training, and offers a brief intro call before you commit.
Ask one more thing: how often will you see that primary clinician, and what happens when they go on vacation? Continuity is part of quality. If your therapist rotates every three weeks, you will spend half of every session re-explaining your life, which is exhausting and clinically unhelpful.
This question takes 90 seconds to ask and tells you more about the program's actual operating model than any brochure.
Question 3: Can you prescribe and manage medication for alcohol use disorder?
Many programs cannot. Many will not say so directly. Ask plainly: do you have a prescriber on staff who manages medication for alcohol use disorder, or do you coordinate with an outside physician?
This matters because three FDA-approved medications exist for alcohol use disorder, and they are underused in community treatment. The American Psychiatric Association practice guideline supports pharmacological treatment alongside psychosocial care as a standard option, not an exotic add-on.4,15
The three medications, named by SAMHSA, are:4
- Naltrexone — reduces cravings and the rewarding effect of drinking. Available as a daily pill or a monthly injection.
- Acamprosate — helps stabilize brain chemistry after you have stopped drinking, reducing the discomfort that drives early return to use.
- Disulfiram — creates an unpleasant physical reaction if you drink, used selectively for motivated patients who want a hard external stop.
None of these are a substitute for therapy. All of them are tools a prescriber can offer if they fit your situation. The APA guideline frames these as legitimate first-line options to discuss.15
A strong answer: "Our medical director can evaluate you for naltrexone or acamprosate during the first two weeks if it makes clinical sense, and we manage the prescription in-house." A weak answer: "We focus on the therapy side and can refer you out if you want to explore that."
Referring out is not disqualifying. But it adds a layer — a separate appointment, a separate copay, a separate clinician who does not see your therapy notes. For a busy professional, in-house medication management is a meaningful convenience and a sign the program treats AUD as a medical condition, not just a behavioral one.
Question 4: How do you treat anxiety, depression, or trauma alongside drinking?
Most people seeking alcohol treatment are also carrying something else. Anxiety. Depression. Sleep that fell apart years ago. A loss that never got worked through. The NIAAA FAQ is direct: co-occurring conditions are common and should be treated at the same time as the drinking concern, not sequenced one after the other.9
Ask how the program handles this. Specifically: is the same clinician treating both, or are there two clinicians coordinating? Is there a psychiatrist available for medication evaluation if your anxiety or depression needs it? Does the treatment plan name your co-occurring concerns explicitly, or does it focus only on drinking and hope the rest resolves?
A strong answer describes integrated care: one treatment plan, two or three issues addressed in parallel, regular communication between therapist and prescriber. A weak answer suggests you "focus on the drinking first" and revisit the rest later. That sequencing rarely works. The anxiety that drove the drinking does not politely wait its turn.9
There is a second reason to push on this. If you are a professional whose mental health is part of why drinking became unmanageable, you need a clinician who can hold both threads. A program that treats only the alcohol side is doing half the work, and the other half is the half that usually causes the return to drinking.
Question 5: How will you tailor the plan to my schedule, privacy, and obligations?
This is the question that separates programs built for working professionals from programs that assume everyone can take a month off.
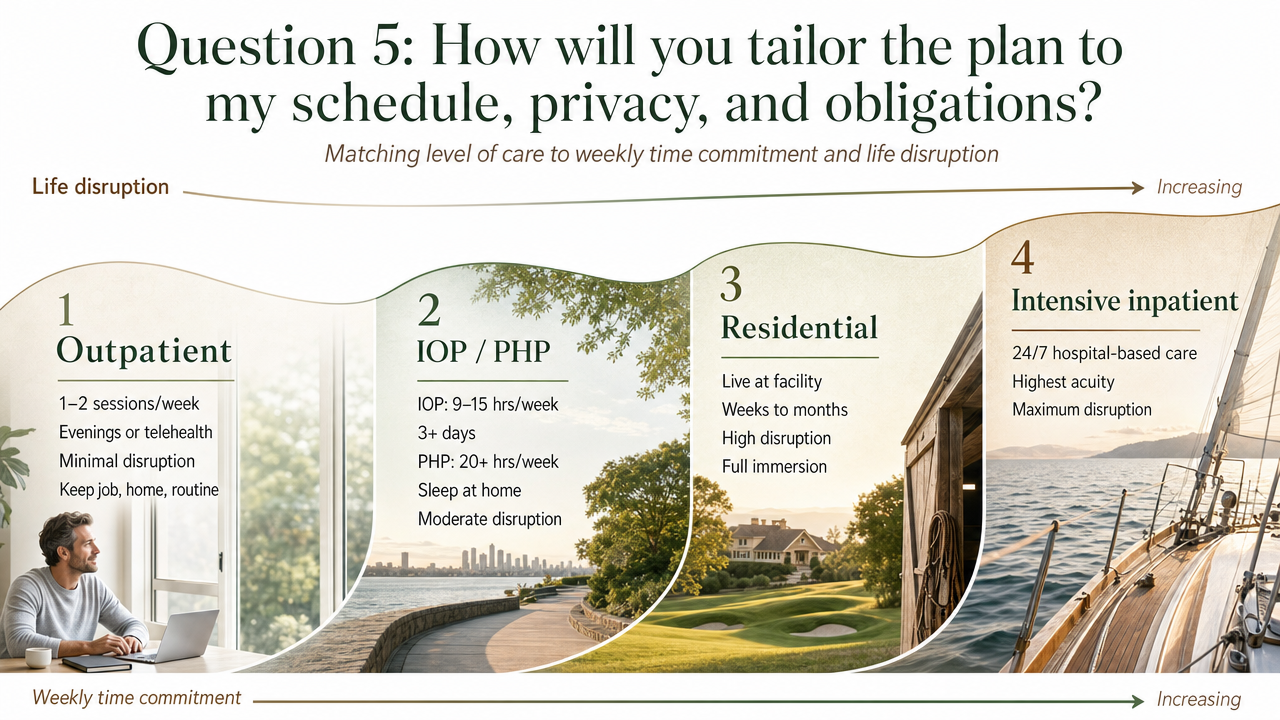
Start with level of care. NIAAA and SAMHSA describe four main levels, and they sit on a spectrum of weekly time commitment and life disruption:1,3
- Outpatient — typically one to two sessions per week, often evenings or telehealth. Minimal disruption. You keep your job, your home, your routine.
- Intensive outpatient (IOP) / partial hospitalization (PHP) — IOP runs roughly 9 to 15 hours per week across three or more days. PHP is more intensive, often 20+ hours per week, but you sleep at home. Moderate disruption.
- Residential — you live at the facility for weeks to months. High disruption to work and family, but full immersion.
- Intensive inpatient — hospital-based, medically supervised, typically short-term for acute medical needs like complicated withdrawal.
A quality program will not push you toward the highest level by default. It will assess your severity, medical risk, and home support, then recommend the lowest level of care that safely treats you. For many working professionals without complicated medical withdrawal risk, that is outpatient or IOP, often with a telehealth component.1,8,12
Then ask the privacy questions. Can sessions be held on telehealth? Are evening or early morning slots available? How are records handled if your licensing board, employer, or insurance ever requests information? Is there a sliding-scale or self-pay path that keeps the visit off insurance entirely?
A strong answer respects that your professional life is part of the clinical picture, not an obstacle to it. A weak answer treats your schedule as a willpower test.
Question 6: How do you measure progress and define success?
Ask the program what success looks like in their own words. Then ask what they actually track.
Good programs measure things. Engagement, retention, session attendance, mood and craving scores over time, return-to-drinking events, quality-of-life check-ins. The research is clear that programs which monitor outcomes and adjust care based on what they see tend to produce better results than programs that do not. Engagement and retention specifically correlate with better long-term abstinence and quality of life.5
A strong answer might sound like: "Every four weeks we review your treatment plan with you, look at attendance, craving scores, and any drinking events, and decide together whether to keep going, step up, or step down." A weak answer reframes the question as a values statement — "success is whatever recovery means to you" — without naming a single thing they actually count.
Also ask how the program defines success itself. Some define it as full abstinence. Others define it as reduced drinking, harm reduction, or improvement in functioning. Both are legitimate clinical positions, but you want to know which one the program holds, because it shapes how they will respond if you have a slip three months in.5
You are asking, in effect, whether the program will notice if you are not getting better. The ones that measure will. The ones that do not, will not.
Question 7: What does this cost, and what does my insurance actually cover?
Save this for last on the call, but do not skip it. A quality program will walk you through cost without flinching.
Ask four things. First, what is the typical length of care for someone in my situation — six weeks, twelve weeks, six months? Second, what is the total expected cost across that length, including therapy, any medication management, and any required group sessions? Third, which insurance plans do you accept, and what is your in-network status with mine? Fourth, do you offer sliding-scale fees, payment plans, or a discreet self-pay option that does not route through insurance?
NIAAA explicitly recommends that providers help you understand course length, accepted insurance, payment options, and sliding-scale fees, and suggests you compare programs "apples to apples" rather than on the sticker price of any one service.7
This last point matters more than it sounds. One program quoting $400 per session for 12 sessions ($4,800) and another quoting a $7,500 flat fee for a 16-week program are not directly comparable until you account for what each includes — therapy frequency, medication management, group sessions, aftercare, family sessions.7
For privacy reasons, some professionals prefer self-pay even when insurance would cover care, because it keeps the diagnosis off the insurance record. A program that handles this conversation matter-of-factly, with clear numbers and clear options, is one that has worked with people in your position before. A program that gets vague about cost is one you should not commit to.
Insight Beyond Treatment
At Next Level Wellness & Behavioral Health, we believe meaningful change starts with perspective, not just protocols.
That philosophy is directly led by Amanda Marino, whose voice in behavioral health extends beyond clinical settings into leadership, culture, and personal growth.
Through keynote speaking and live events, Amanda explores the deeper themes that show up in recovery, family systems, and life transitions: authenticity, resilience, accountability, and the courage to change. Her work invites audiences to move past labels and into honest conversations that create lasting impact.
Strong answers vs. weak answers: what to listen for
By the third intake call, the language starts to blur. Every program sounds caring. Every program says it individualizes care. The difference is what they say next.
Here is the contrast across all seven questions, pulled from the NIAAA framework for what high-quality answers actually sound like;13,18
On therapies. Strong: "We use CBT and motivational enhancement therapy, delivered by our two licensed clinical social workers, over 12 to 16 weekly sessions." Weak: "We take a holistic, integrated approach customized to each client."
On credentials. Strong: "You'd work with Dr. Chen, a licensed psychologist with addiction certification. Here's her bio. She's out the first week of August; Dr. Patel covers." Weak: "Our whole team is highly qualified and you'll be matched with the right fit."
On medication. Strong: "Our medical director evaluates every client for naltrexone or acamprosate in the first two weeks. We prescribe and monitor in-house." Weak: "We're more focused on the underlying issues, but we can refer out if you're interested."
On co-occurring conditions. Strong: "One treatment plan addresses your anxiety and drinking together. Your therapist and prescriber meet biweekly to coordinate." Weak: "Let's get the drinking stable first, then look at the anxiety."
On schedule and privacy. Strong: "We offer Tuesday and Thursday evening telehealth groups, plus a self-pay option that stays off your insurance record." Weak: "Recovery has to come first — you'll need to make the time."
On outcomes. Strong: "We review attendance, craving scores, and any drinking events every four weeks and adjust the plan with you." Weak: "Success looks different for everyone."
On cost. Strong: "Twelve weeks of weekly therapy plus medication management runs roughly X. Here's what your insurance covers, here's the sliding-scale option, here's self-pay." Weak: "It depends on a lot of factors — we can talk numbers after the assessment."
You are listening for nouns and numbers. When you hear them, write them down. When you do not, that is also data.
Where to search without giving up your privacy
Skip the search engine ads. The first three results are almost always paid placements from large marketing networks, not the programs themselves. Use vetted directories instead.
Start with FindTreatment.gov, SAMHSA's confidential locator. You can filter by location, level of care, payment type, and telehealth availability without creating an account or leaving identifying information. The NIAAA Alcohol Treatment Navigator runs a parallel directory specifically for alcohol care, organized so you can compare specialty physicians, therapists, and programs side by side. Both tools were built to route you around the marketing layer.2,6
For referrals that never touch a search history, ask your primary care physician or a trusted therapist for two or three names. Clinicians often keep informal short lists of local providers they trust, and a peer-to-peer handoff carries weight on the intake call. State health departments and county councils on alcohol concerns also maintain directories of licensed programs, which is useful if you want to verify a provider's standing independent of how they present themselves online.10,14
When you make the call, you do not have to use your full name on the first pass. "First name only for now" is a normal request, and a quality program will not push back.
Making the first call
The first call is the hardest one. After that, the script gets easier.
Pick a time when you will not be interrupted for 20 minutes. Close the door. Have a glass of water and a notepad. You do not need to rehearse a story. You need a sentence about what you want and seven questions in front of you.
If you freeze, the SAMHSA National Helpline at 1-800-662-HELP (4357) is free, confidential, and staffed 24 hours a day, 365 days a year. They do not run a treatment program. They listen, refer, and help you think through next steps in your state and your insurance situation. Using the helpline is not a commitment. It is a way to make the second call easier.11
A few things to remember while you dial. You are allowed to take notes. You are allowed to ask a clinician to slow down or repeat an answer. You are allowed to say "I need to think about this" and call back tomorrow. The decision you are making deserves more than five minutes, and a program that respects that will give you the time.
Making this call is hard. Asking these seven questions makes the next call easier, and the one after that easier still.
For support that meets you right where you are—anytime, anywhere—connect with us today.
Frequently Asked Questions
Is outpatient alcohol treatment as effective as residential rehab for a working professional?
For many people without complicated medical withdrawal risk, yes. Well-designed outpatient care delivers the same evidence-based therapies and medications used in residential settings, with far less disruption to work and family. A clinician with addiction training should evaluate your severity and home support before recommending a level of care, and the goal is the lowest level that safely treats you.8,12
Can I get alcohol treatment entirely through telehealth?
Often, yes. Since 2020, far more providers offer alcohol care by phone or video, and some accredited programs operate fully through telehealth. The NIAAA Navigator suggests asking directly about video or phone session availability when you compare providers. Telehealth can include individual therapy, group sessions, and medication management visits with a prescriber, which preserves privacy and protects your schedule.1,2
What medications are approved for alcohol use disorder, and should I ask about them?
Three FDA-approved medications exist: naltrexone, acamprosate, and disulfiram. Naltrexone reduces cravings, acamprosate stabilizes brain chemistry after you stop drinking, and disulfiram creates a deterrent reaction if you drink. The American Psychiatric Association practice guideline supports these as legitimate options alongside therapy, not exotic add-ons. Ask every program whether they prescribe in-house or refer out.4,15
How do I protect my privacy and professional license while in treatment?
Ask the program directly how records are handled and whether a self-pay option exists that keeps the diagnosis off your insurance record. Telehealth sessions remove the visible visit to a clinic. Use trusted directories like FindTreatment.gov rather than search engine ads, which can collect identifying information. On the first call, first-name-only is a normal request a quality program will honor.6,7
Does insurance actually cover alcohol treatment, and how do I compare costs across providers?
Most health insurance covers some alcohol treatment under behavioral health benefits, though coverage varies. To compare apples to apples, ask each program for the typical length of care, total expected cost across that length, in-network status with your plan, and whether sliding-scale or self-pay options exist. A program that gets vague about cost is one to skip.7
What if I need help right now, before I finish vetting programs?
Call the SAMHSA National Helpline at 1-800-662-HELP (4357). It is free, confidential, and staffed 24 hours a day, 365 days a year, for treatment referral and information. The helpline does not run a program, so there is no sales pressure. They can help you think through next steps in your state and your insurance situation while you continue comparing providers.11
References
- What Types of Alcohol Treatment Are Available?. https://alcoholtreatment.niaaa.nih.gov/what-to-know/types-of-alcohol-treatment
- Step 1 - SEARCH Trusted Sources To Find Providers. https://alcoholtreatment.niaaa.nih.gov/how-to-find-alcohol-treatment/step-1-search-trusted-sources-to-find-providers
- Treatment Types for Mental Health, Drugs and Alcohol. https://www.samhsa.gov/find-support/learn-about-treatment/types-of-treatment
- Treatment Options for Substance Use Disorder. https://www.samhsa.gov/substance-use/treatment/options
- Substance Use Disorder Treatment Outcomes. https://pmc.ncbi.nlm.nih.gov/articles/PMC12180564/
- Substance Use Disorders Treatment Options - SAMHSA Blog. https://www.samhsa.gov/blog/substance-use-disorders-treatment-options
- What About Costs and Insurance. https://alcoholtreatment.niaaa.nih.gov/what-to-know/costs-and-insurance
- Why Do Different People Need Different Options?. https://alcoholtreatment.niaaa.nih.gov/what-to-know/different-people-different-options
- Frequently Asked Questions: Searching for Alcohol Treatment. https://alcoholtreatment.niaaa.nih.gov/FAQs-searching-alcohol-treatment
- For Healthcare Professionals - NIAAA Alcohol Treatment Navigator. https://alcoholtreatment.niaaa.nih.gov/healthcare-professionals
- National Helpline for Mental Health, Drug, Alcohol Issues - SAMHSA. https://www.samhsa.gov/find-help/helplines/national-helpline
- Outpatient Treatment of Alcohol Use Disorder. https://meded.dom.pitt.edu/wp-content/uploads/2023/11/Outpatient-Treatment-of-Alcohol-Use-Disorder-Spinella-UIM-2023.pdf
- Q&As for Alcohol Treatment Programs. https://alcoholtreatment.niaaa.nih.gov/how-to-find-alcohol-treatment/10-questions-for-alcohol-treatment-programs
- Chapter 5—Specialized Substance Abuse Treatment Programs (Treatment Improvement Protocol Series). https://www.ncbi.nlm.nih.gov/books/NBK64815/
- The American Psychiatric Association Practice Guideline for the Pharmacological Treatment of Patients With Alcohol Use Disorder. https://pubmed.ncbi.nlm.nih.gov/29301420/
- Alcohol Facts and Statistics (NIAAA). https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/alcohol-facts-and-statistics
- Substance Use Disorders: Statutes, Regulations, and Guidelines. https://www.samhsa.gov/substance-use/treatment/statutes-regulations-guidelines
- Step 2 – Ask 10 Recommended Questions. https://alcoholtreatment.niaaa.nih.gov/how-to-find-alcohol-treatment/how-to-search-what-to-ask/step-2-ask-10-recommended-questions
A Voice Shaping the Conversation
The topics explored here—change, self-awareness, recovery, and growth—are the same themes Amanda Marino brings to audiences nationwide through speaking engagements and live events.
Known for her appearances on A&E’s Intervention and Digital Addiction, Amanda speaks to organizations, communities, and leadership teams about navigating adversity, embracing vulnerability, and building lives rooted in purpose. Her message resonates far beyond treatment, offering insight that applies to families, professionals, and anyone standing at a crossroads.



Heal on your terms—any time, anywhere.